A public figure can know the exact moment treatment becomes necessary and still delay it for weeks. The reason usually isn't denial alone. It's logistics. A founder has investors waiting on a call. A performer has contractual appearances. A physician or attorney has people depending on decisions that can't disappear for a month.
That's why luxury private rehab for celebrities exists in a category of its own. It isn't ordinary residential care with better furniture. It's a clinical setting built for people whose recovery has to happen alongside privacy demands, reputation risk, and carefully limited professional continuity. For executives, C-suite leaders, and high-achieving professionals, that difference matters.
The right program protects treatment first. It also understands reality. Some residents need private rooms in detox and residential treatment, tightly structured access to laptops and cell phones, and a clinical team that can treat trauma, anxiety, mood instability, and substance use at the same time without turning recovery into a public event or a career collapse.
The Professional's Dilemma Finding Help Without Hitting Pause
By the time many high performers start searching, life has already narrowed. Sleep is unstable. Alcohol, stimulants, prescription medications, or other substances have moved from stress management to daily dependence. Mood symptoms are getting harder to hide. Assistants, spouses, managers, or legal counsel may know something is wrong, but the person at the center of it still believes treatment means stepping away from everything that defines them.
That assumption keeps people stuck.
A celebrity may fear one leaked admission. A C-suite executive may fear a board-level ripple effect. A working professional may fear that silence during treatment will create more damage than the problem itself. That's why standard advice often falls flat. “Just unplug” sounds simple to people who don't carry payroll, contracts, public visibility, or a family system built around their availability.
For this population, treatment has to be private, clinically serious, and operationally realistic. Programs built for working professionals in treatment address that reality directly. They don't treat career obligations as vanity. They treat them as part of the pressure system that has to be managed correctly if recovery is going to hold.
Excess responsibility often becomes part of the illness pattern. Good treatment doesn't pretend that pressure doesn't exist. It teaches the resident how to stop being ruled by it.
The central dilemma isn't whether help is needed. It's whether help can happen without public exposure, unnecessary chaos, or a complete professional shutdown. High-end private pay rehab answers that by building treatment around discretion, private accommodations, and clinical structure strong enough to support both stabilization and carefully bounded outside contact.
Defining the Elite Rehab Experience
You can be in treatment and still carry real responsibility. The program has to be designed for that reality from the first day.
Luxury earns its place only when it improves clinical care. In an elite setting, that means strict privacy, physical conditions that settle the nervous system, and a treatment model that can absorb the demands of a high-stakes career without letting work take over recovery.

Privacy is part of treatment
High-profile clients need containment, not attention. A serious private rehab program limits exposure, controls access, protects identity, and removes the social friction that can interfere with detox, sleep, psychiatric stabilization, and honest participation in therapy.
Private rooms matter for clinical reasons. Withdrawal is messy. Trauma work is exposing. Medication changes can affect mood, sleep, and concentration. Shared living can increase stress at the exact point where a patient needs less stimulation and more control. That is also why careful psychiatric medication management belongs inside the treatment plan, not as an afterthought.
The setting should reduce strain, not show off
Accomplished clients often arrive overstimulated, sleep-deprived, guarded, and used to controlling every variable around them. The environment should lower that load quickly. Quiet private space, predictable routines, quality food, and orderly design help residents settle faster and stop wasting energy on avoidable discomfort.
That is not vanity. It is good clinical judgment.
The same principles shape other elite residential environments built around controlled access and discretion. Readers who want a useful comparison can review Penthouse Agents' celebrity penthouses analysis.
Clinical sophistication separates real treatment from expensive hospitality
This is the line that matters most. Beautiful surroundings support recovery. They do not diagnose bipolar disorder, manage complicated detox, treat trauma, or address the habits that keep high performers outwardly functional and privately unwell.
Elite care should feel individually built because it is. The schedule, level of outside contact, psychiatric oversight, family work, and recovery planning should reflect the patient's actual risks and obligations. For celebrities, founders, physicians, attorneys, and executives, electronics access and professional communication should be structured as a clinical decision. Used well, they become part of therapy. Used poorly, they keep the old pressure cycle alive inside treatment.
A strong program usually includes:
- Private accommodations across levels of care so stabilization happens with less exposure and fewer unnecessary stressors.
- Individualized treatment planning that addresses substance use alongside anxiety, depression, trauma, burnout, sleep disruption, grief, or mood symptoms.
- Structured policies for phones, laptops, and work contact so professional obligations are handled in a controlled way, with boundaries that protect treatment time.
- Private pay flexibility that supports more individualized scheduling, closer staffing, and a level of discretion insurance-driven programs often cannot provide.
Bottom line: If a program can describe the thread count better than its psychiatric model, it is selling comfort instead of treatment.
The Cornerstone of Clinical Excellence in Treatment
High achievers often enter treatment with a simple request. Keep me clinically safe, keep this private, and help me protect what can be protected at work without letting work keep me sick. A top-tier program can do that, but only if clinical depth leads every decision.
The most expensive mistake families make is paying for privacy and comfort without confirming medical and psychiatric capability. Beautiful surroundings help people settle. They do not diagnose bipolar disorder, stabilize a complicated withdrawal, or treat the anxiety, trauma, burnout, and depression that often sit underneath substance use.
For celebrities, executives, physicians, founders, and public figures, the clinical picture is rarely clean or single-layered. Many have spent years performing well under pressure while sleep erodes, mood becomes less predictable, relationships tighten, and substances become the tool that keeps the machine running. Once that tool is removed, the underlying symptoms do not disappear. They become easier to see.
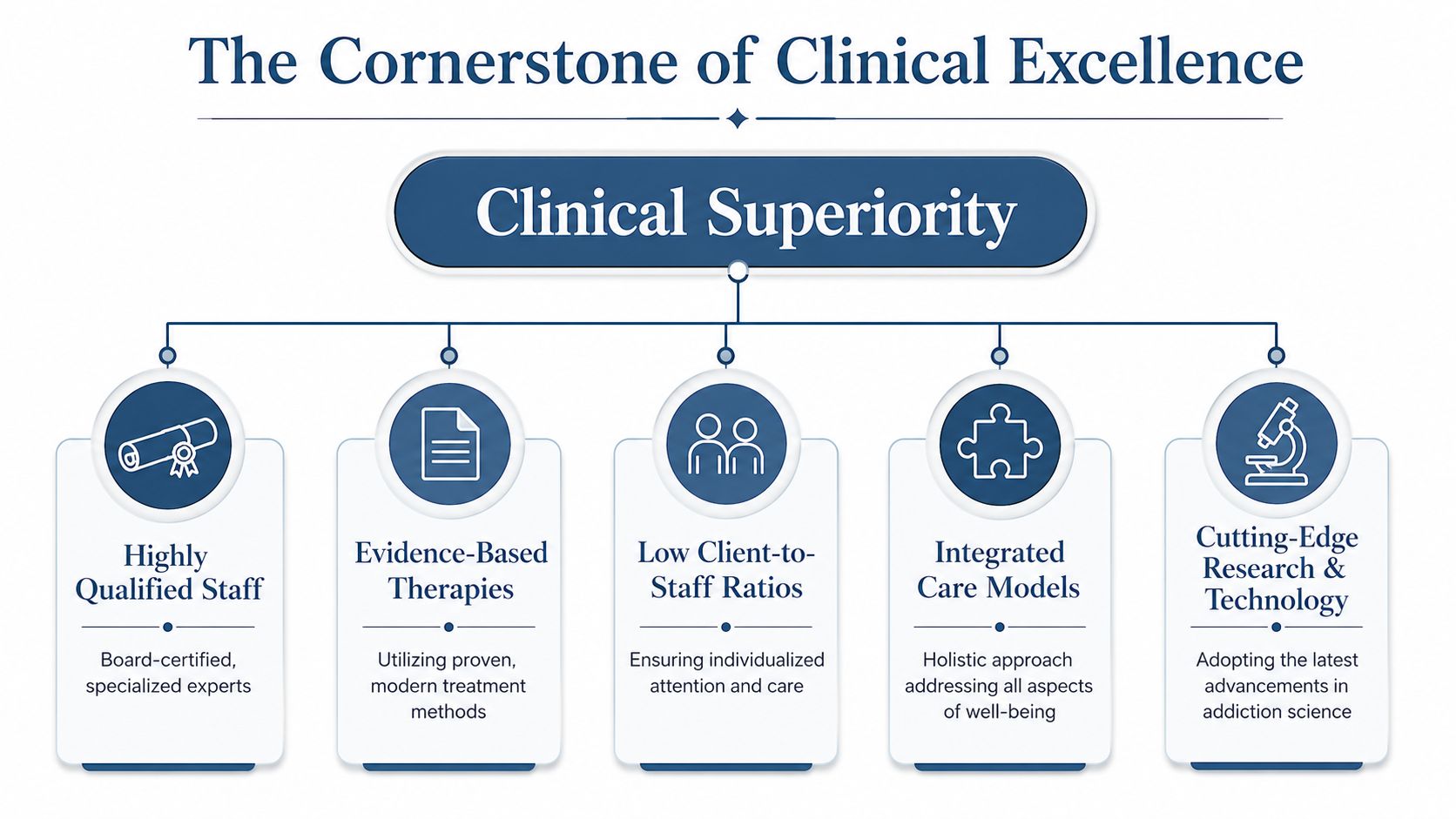
Dual diagnosis has to be built into treatment
A program that separates addiction treatment from mental health treatment usually creates short-term stabilization and little else. If trauma, panic, mood instability, grief, or obsessive pressure patterns are left untreated, the resident often returns to the same internal conditions that supported substance use in the first place.
Clinical sophistication is the true dividing line. The team should be able to assess substance use, psychiatric symptoms, sleep disruption, trauma history, and work-related stress as one connected problem, then build a treatment plan that reflects that reality. For a high-profile client, this also includes structured decisions about phone access, laptop use, and professional communication. Those boundaries belong inside the clinical plan because they affect stress, avoidance, sleep, and relapse risk.
Medication strategy matters here. A resident may arrive overmedicated, undermedicated, or taking prescriptions that made sense during crisis but no longer fit the full picture. Careful psychiatric medication management in treatment should be integrated with therapy, detox oversight, and daily observation. It should never function as a disconnected side service.
What strong clinical staffing actually changes
Luxury only means something if the staffing model can respond fast and intelligently. That requires psychiatrists, medical providers, licensed therapists, and addiction clinicians working from the same treatment plan and updating it as the resident stabilizes.
Weak staffing misses patterns. Strong staffing catches them early.
| Clinical issue | Weak staffing response | Strong staffing response |
|---|---|---|
| Escalating anxiety | Resident is told to “use coping skills” | Psychiatric and therapeutic intervention happen quickly |
| Trauma activation | Symptoms are misread as resistance | Team adjusts pace, modality, and safety planning |
| Early relapse thinking | Concern is noticed late | One-on-one work addresses it before discharge planning stalls |
For clients with active careers, staffing depth also determines whether professional obligations are handled in a therapeutic way or allowed to sabotage treatment. If a resident needs limited contact with an agent, attorney, business partner, or assistant, the team should set clear windows, define the purpose of contact, and review the emotional impact afterward. That is not concierge service. It is clinical containment.
What to ask before admission
Families, attorneys, and trusted advisors should press for specifics.
- Ask who is diagnosing and directing care. You want psychiatrists, doctoral-level clinicians, and licensed therapists with clear dual-diagnosis experience.
- Ask how withdrawal and psychiatric symptoms are distinguished. Early treatment goes badly when a program confuses detox effects with mood or trauma disorders, or misses the opposite.
- Ask how the team handles electronics and work contact. The answer should include structure, timing, clinical review, and boundaries. “Case by case” is not enough.
- Ask how trauma treatment is paced. Good programs can explain what they do, when they do it, and how they avoid flooding a resident who is still stabilizing.
The right question is straightforward. Can this team treat addiction, mental health symptoms, and the pressures of a high-stakes career as one integrated clinical problem? If the answer is vague, keep looking.
Personalized Programs A Day in Treatment
You can tell within the first 24 hours whether a program is built for real recovery or for appearances. A serious center runs on clinical rhythm. The day feels calm, private, and purposeful. Every hour has a reason.
For a public figure, founder, studio executive, or trial attorney, that matters. Early treatment is rarely derailed by lack of insight alone. It is derailed by overstimulation, poor sleep, unmanaged withdrawal, image anxiety, and constant pressure to stay available. High-end residential care should reduce that noise fast so the resident can stabilize and effectively absorb treatment.
A private room helps. So does a setting with low census, experienced nursing, and enough one-to-one time that care is adjusted in real time rather than forced into a generic schedule.
What a representative day may include
A good day in treatment is personalized, but it is not loose. Structure creates safety. Personalization makes the structure clinically useful.
The morning often starts with a medical or psychiatric check-in, especially early in the stay when sleep, appetite, mood shifts, cravings, and medication response need close review. From there, the resident moves into individual therapy focused on the issues driving use now, not just the history behind it.
The rest of the day may include:
- Individual psychotherapy for substance use, trauma, anxiety, depression, grief, burnout, or relationship damage.
- Small process or skills groups using CBT, DBT, ACT, motivational interviewing, or relapse-prevention work.
- Body-based and experiential sessions such as fitness, mindfulness, somatic therapies, art, or equine work when they fit the treatment plan.
- Case management and family work to address legal, financial, relational, or household problems that can destabilize recovery after discharge.
- Structured professional contact, when clinically appropriate, with defined time blocks for urgent communication that the treatment team can frame, monitor, and review afterward.
That last point deserves more attention than it usually gets. In elite rehab, limited work access should be treated the same way the team treats medication changes or trauma pacing. It needs a plan. If a resident must answer a time-sensitive production issue, prepare for board communication, or maintain public-facing composure with expert media interview preparation, that contact belongs inside the treatment framework. It should never turn the residence into a disguised office.
This visual gives a sense of the residential setting such care can happen in.
Luxury should support treatment, not distract from it
Comfort has clinical value when it lowers stress and supports regulation. Good food, privacy, restorative sleep, movement, and carefully chosen experiential therapies can help a resident settle enough to do difficult psychological work. They should be used with intent.
Art therapy after an emotionally demanding session can help a resident process without shutting down. Fitness can restore routine, improve mood, and rebuild confidence in a body that has been neglected or overdriven. Mindfulness can reduce reactivity before family work or professional check-ins. Used this way, amenities support treatment. Used poorly, they become polished avoidance.
That distinction matters.
What families and advisors should expect
Privacy should never mean silence or drift. The best programs keep confidentiality intact while still giving families, attorneys, and trusted advisors a clear picture of how the plan is progressing.
Expect a few basics:
- Clinical privacy is protected. Personal disclosures stay in treatment.
- Family involvement is purposeful. Contact happens because it improves communication, accountability, or discharge planning.
- The schedule changes when the resident changes. A strong team adjusts intensity, pacing, and outside contact based on clinical progress.
- Aftercare planning starts early. Return-to-work strategy, psychiatric follow-up, relapse planning, and communication boundaries should be built before discharge, not discussed on the last day.
Cost reflects that level of staffing and customization. You are paying for time, discretion, clinical depth, and the ability to build a treatment day around one person's risks and responsibilities rather than around institutional convenience.
Balancing Recovery and Professional Life
Your company can survive a delayed reply. Your recovery will not survive a treatment program that turns into a disguised workday.
High-performing professionals do better in rehab when work contact is handled as part of the clinical plan, not sold as a luxury feature. Phones and laptops belong in treatment only when the team can show why access helps this specific resident stay engaged, regulated, and honest. If device use feeds panic, image control, compulsive checking, or late-night stimulation, access should narrow quickly.
Electronics need a treatment plan
A serious executive track sets rules that match the resident's psychiatric stability, relapse history, and actual job demands. That usually means scheduled communication windows, private space for time-limited calls, and clinical review of what happened before and after each work block. The point is not convenience. The point is to keep outside obligations from hijacking treatment.
This approach protects two things at once. It protects the resident's concentration in therapy, and it protects the business from impulsive decisions made in withdrawal, shame, or sleep deprivation.
What healthy work continuity actually looks like
Residents with high-stakes roles often need to approve a narrow set of decisions, speak with counsel, or reassure a small circle of key people. Fine. Put boundaries around it.
A workable structure often includes:
- Defined device hours instead of open access all day
- A short list of approved contacts rather than constant availability
- Private, monitored work periods that do not interfere with groups, psychiatry, or sleep
- Clinical review of work behavior to separate duty from avoidance
- Immediate tightening of access if communication increases agitation or undermines treatment
That is the standard to look for. If a program cannot explain exactly how electronics are managed, it is not running an executive track. It is handing a stressed resident the same coping mechanism that helped drive the crash.
Public-facing professionals need another layer of planning. Returning to interviews, investor meetings, or press attention right after treatment can trigger the same performance reflexes that kept the problem hidden. Clinical work should cover disclosure boundaries, stress responses, and rehearsal for high-pressure communication. Separate professional support can help with presentation skills, and some clients also use expert media interview preparation after discharge.
Cost and coverage matter here because executive accommodations, private space, and added clinical coordination can change what is billed and what is not. Review your insurance coverage for addiction treatment early, before admissions promises turn into avoidable financial friction.
Vetting a Program and Understanding Costs
You may be choosing care while a publicist is asking for dates, a board is waiting for an answer, and your family wants certainty by tonight. That pressure makes polished admissions calls dangerous. A luxury setting can calm nerves, but it can also hide thin clinical staffing, weak psychiatric coverage, and vague policies around privacy, work access, and discharge.

What deserves a direct answer
Treat admissions like a due diligence call. Ask specific questions. Write down the answers. If the conversation keeps drifting back to chef-prepared meals, ocean views, or exclusivity, you are hearing marketing, not a treatment plan.
A credible program should explain these points without hesitation:
- Accreditation and licensing. Confirm state licensure and recognized accreditation.
- Psychiatric coverage. Ask who evaluates mood, trauma, anxiety, sleep, and substance use, and how often that clinician sees residents.
- Therapy delivery. Ask which licensed clinicians provide individual therapy, group therapy, and family work.
- Dual-diagnosis treatment. Ask how the program treats addiction and mental health conditions together, not in parallel.
- Private accommodations. Confirm whether private rooms are available in detox and residential care if privacy is a requirement.
- Work and electronics structure. Ask for the actual protocol. Who approves access, when devices are used, where work happens, and what causes access to tighten.
- Discharge planning. Ask what support is arranged before a resident leaves, including psychiatry, therapy, relapse planning, and return-to-work preparation.
Cost deserves the same discipline. In private rehab, price can reflect privacy, staffing, medical complexity, length of stay, and how much individual care is built into the schedule. It can also reflect pure hospitality. You need to know which one you are paying for.
Red flags that should stop the conversation
Some warning signs are immediate.
| Red flag | Why it matters |
|---|---|
| Luxury is described in detail, treatment is vague | The sales story is stronger than the clinical model |
| No clear explanation of psychiatric care | Mood symptoms, trauma, or anxiety may be missed or under-treated |
| Phone and laptop access is sold as unrestricted convenience | Work may be driving treatment instead of being contained within it |
| Admissions cannot explain who is on site each day | Staffing may be thinner than advertised |
| Discharge planning starts after admission | The program may be reactive instead of organized |
Insurance may still play a role, even in private-pay settings. Before you commit, review insurance coverage for addiction treatment so you understand what may be reimbursable, what is not, and where executive or privacy-related costs fall outside coverage.
One factual example can be stated plainly. Reflections is a California-licensed, Joint Commission-accredited luxury rehabilitation provider offering private rooms, dual-diagnosis care, and clinically appropriate electronics access for adults who need to balance treatment with ongoing responsibilities.
A serious program should be able to explain exactly what the resident is paying for, clinically and operationally, in clear language.
Your Path to Discreet and Lasting Recovery
The right luxury private rehab program does three things at once. It protects privacy, delivers real psychiatric and addiction treatment, and respects the fact that high-achieving people often can't disappear from life without a plan.
That combination is what separates genuine elite care from expensive window dressing. Private rooms matter. Discretion matters. Structured access to phones and laptops matters for some residents. But none of it counts unless the program can also treat trauma, mood symptoms, anxiety, and substance use with consistency and skill.
For celebrities, executives, C-suite leaders, and working professionals, the best decision is usually the clearest one. Choose a private pay program that can describe its clinical model in detail, explain its electronics boundaries without hesitation, and support career continuity without letting work consume treatment.
The next step doesn't need to be public, dramatic, or final. It only needs to be confidential and informed.
Reflections offers confidential consultations for adults seeking private, high-end dual-diagnosis treatment in a luxury residential setting. Those exploring options for discreet rehab, private detox, or an executive track that includes clinically managed access to phones and laptops can learn more through Reflections.









