A senior executive usually recognizes the pattern before anyone else does. Sleep gets shorter. Decisions take longer. Patience thins out at home and at work. A glass of wine becomes several, or an as-needed prescription starts carrying more of the week than it should. The problem isn't insight. It's the fear that getting help will interrupt everything that has taken years to build.
That fear is one reason psychiatric medication management matters in a residential setting designed for executives, founders, physicians, attorneys, and other high-responsibility professionals. The right approach isn't blunt, sedating, or disconnected from real life. It's deliberate. It aims to stabilize mood, reduce suffering, protect cognitive performance, and fit inside a treatment plan that respects privacy, discretion, and ongoing professional obligations.
For high-functioning adults with co-occurring mental health and substance use concerns, medication decisions need more than a quick prescription pad. They require close psychiatric oversight, strong psychotherapy, and an environment where recovery can proceed without unnecessary chaos. In a private-pay luxury program, that often means small census, private rooms, coordinated care, and enough structure to support healing without forcing a successful professional to vanish from their life.
A Strategic Approach to Mental Wellness for Leaders
Executives often delay treatment because they assume accepting psychiatric help means surrendering control. In practice, the opposite is usually true. A precise medication plan can restore control by reducing agitation, panic, insomnia, depression, impulsivity, or emotional volatility that has already begun to affect judgment and endurance.
Psychiatric medication management works best when it's treated like a strategic intervention, not a generic fix. The clinician's job isn't just to prescribe something for symptoms. The job is to determine what's driving the symptoms, what substances or medical issues may be complicating the picture, and what level of pharmacology is necessary.
Why leaders need precision
A high-performing professional rarely asks, “Will this help me feel something?” The more common question is, “Will this help me function without dulling me?” That's the right question.
In a luxury executive setting, the standard should be:
- Minimal effective pharmacology: enough support to improve stability, not so much that performance, clarity, or motivation are blunted
- Discretion: treatment that protects privacy and limits unnecessary exposure
- Continuity: the ability to stay appropriately connected to pressing work and family responsibilities
- Customization: decisions based on the whole person, not just a diagnosis label
Practical rule: Medication should support the work of recovery, not replace it.
Mental health and physical health also affect one another more than many professionals realize. For readers trying to understand that overlap, this discussion of understanding weight loss and mental well-being is useful because it highlights how stress, mood, behavior, and body regulation can move together instead of separately.
The broader need for thoughtful psychiatric care is clear. Globally, total psychotropic medicine consumption rose from 28.54 DDD per 1000 inhabitants per day in 2008 to 34.77 in 2019, with Northern America at 167.54 and Asia at 5.59 in 2019, according to global psychotropic medicine consumption data. More access to medication can be a good thing, but access alone isn't the same as expert management. For executives, precision matters more than volume.
What Is Psychiatric Medication Management
Psychiatric medication management is an evidence-based process integrating prescribing with ongoing monitoring. It isn't a one-time medication decision. It's a continuing clinical relationship in which a psychiatrist evaluates response, tracks side effects, adjusts dosing, and coordinates medication with the rest of treatment.
A useful analogy is a master watchmaker adjusting a complex instrument. The goal isn't to force movement. It's to restore proper timing, balance, and reliability. In mental health treatment, that can mean helping the brain and body settle enough for sleep to normalize, concentration to improve, anxiety to soften, or mood swings to become manageable.
What the process includes
A sound medication management process usually involves several moving parts:
- Careful selection: the psychiatrist considers symptoms, past medication history, medical issues, substance use, and functional demands
- Monitoring: the team watches for benefits, tolerability, and unintended effects
- Adjustment: dose, timing, or medication choice may change as the patient's response becomes clearer
- Integration with therapy: medication supports the deeper work rather than standing alone
That final point is essential. According to this explanation of why psychiatrists excel in psychiatric medication management, medication management is most effective when combined with psychotherapy because the combination addresses both neurochemical balance and the behavioral patterns contributing to the disorder, producing better long-term outcomes than medication alone.
What it is not
Psychiatric medication management isn't automatic medicating. It also isn't a promise that every symptom should be treated with another prescription. In an advanced residential program, the standard is restraint and judgment.
That matters in practical situations executives already understand. Supply interruptions, prior authorizations, travel schedules, and changing pharmacies can all complicate continuity. Readers dealing with stimulant access issues may find navigating ADHD medication shortages helpful for understanding practical disruptions that can affect even well-established regimens.
For clients with substance use concerns, medication decisions also overlap with recovery planning. In those cases, a related framework is medication-assisted treatment in addiction care, where medications are used selectively and clinically, not casually.
The best medication plan is often the one that does less, but does it consistently and safely.
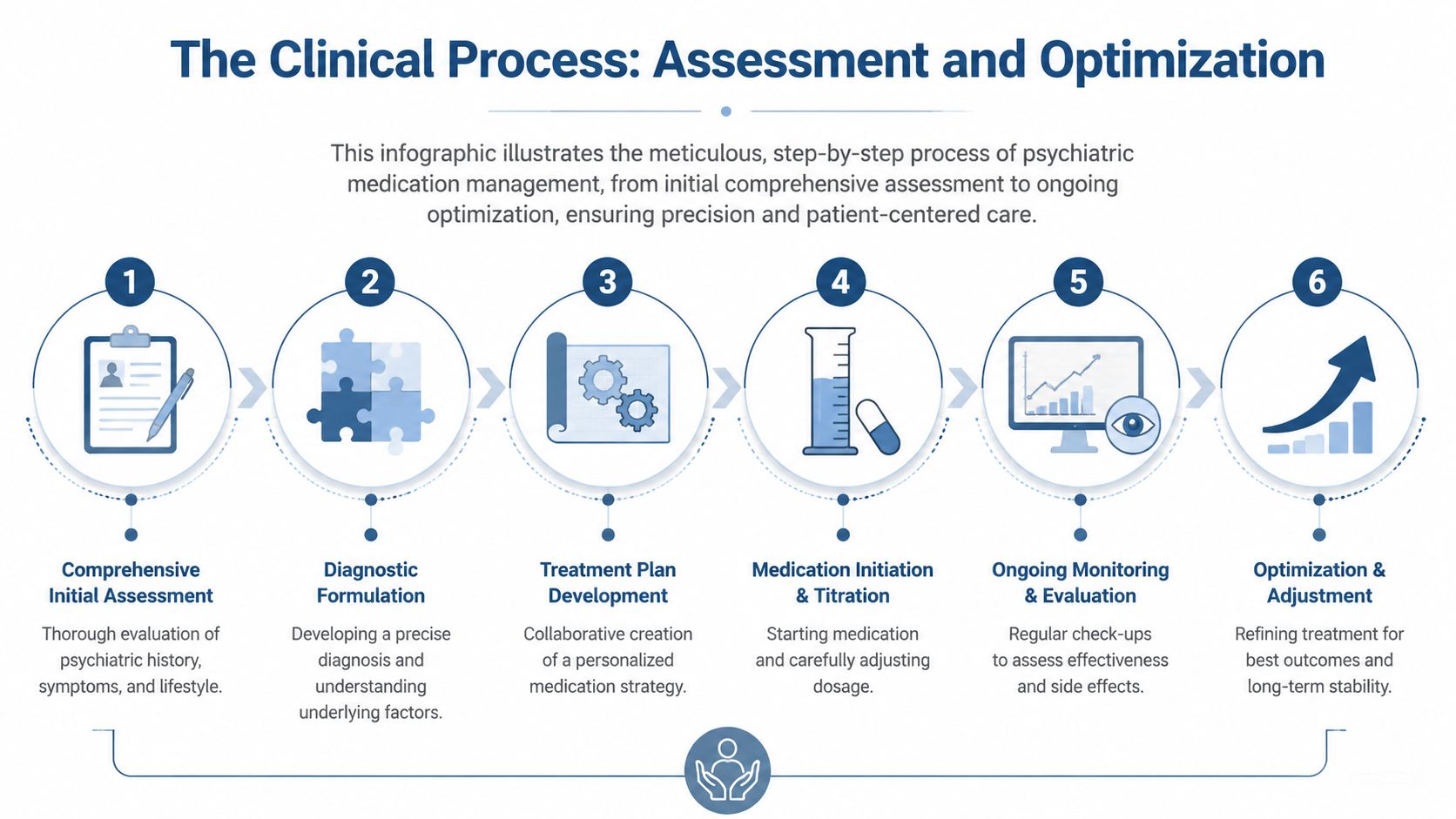
The Clinical Process Assessment and Optimization
Medication management should feel methodical, not mysterious. In a high-end residential environment, that process begins with a full psychiatric and functional assessment, then moves into structured optimization over time.
The first phase
At intake, the psychiatrist isn't only asking about mood or anxiety. The assessment should examine sleep, trauma history, current stressors, alcohol or drug use, prior treatment, family psychiatric history, medical conditions, and the exact way symptoms interfere with work, decision-making, and relationships.
For executives with dual-diagnosis concerns, a deeper front-end evaluation matters. A program that incorporates neuropsychiatric assessment as part of intake for dual diagnosis can clarify whether the presenting problem is primarily depressive, anxiety-driven, trauma-related, substance-induced, bipolar-spectrum, or some combination of several.
Why specialist judgment changes outcomes
A psychiatrist does more than match symptoms to a drug class. The clinical reasoning is more complex than that. Research described in this analysis of psychiatric prescribing frameworks shows that psychiatrists use specialized justification frameworks distinct from general practice. They tailor recommendations to the patient's concerns while also grounding decisions in professional expertise about the patient's likely future mental state. That specialist process reduces adverse outcomes compared with non-specialist care.
For a busy professional, this difference shows up in concrete ways:
| Clinical question | General concern | Specialist focus |
|---|---|---|
| Is the person anxious? | Reduce distress | Determine whether anxiety is primary, trauma-related, withdrawal-related, or part of a mood disorder |
| Is the medication helping? | Ask about symptom relief | Weigh relief against cognition, sleep quality, activation, sedation, and relapse risk |
| Should the dose change? | Increase or maintain | Consider timing, interaction effects, pattern of response, and downstream consequences |
Optimization is where the real work happens
The first prescription is only a starting point. During the early weeks, clinicians watch for symptom movement, side effects, sleep changes, appetite shifts, and any sign that the medication is helping one problem while worsening another.
A strong process often looks like this:
- Start with a hypothesis: choose the narrowest effective intervention based on the assessment.
- Titrate deliberately: small changes often reveal more than aggressive ones.
- Review function, not just symptoms: can the client think clearly, participate in therapy, sleep, and regulate emotions?
- Adjust or simplify: if a medication isn't earning its place, it shouldn't stay by default.
Good psychiatric care doesn't chase every symptom with another pill. It tests a theory, observes carefully, and corrects course.
Navigating Side Effects Risks and Benefits
Most professionals considering treatment ask the same quiet question: will medication make it harder to think, lead, negotiate, or stay sharp? That concern is legitimate. Any psychiatrist working with executives should treat side effects as central to the conversation, not as an afterthought.

The aim is minimal, effective pharmacology. That means using the least medication necessary to achieve meaningful stability and then reassessing whether the regimen still makes sense as sleep improves, withdrawal resolves, therapy deepens, or stress changes.
What good risk management looks like
Medication decisions are always trade-offs. The right question isn't whether a medication has possible downsides. The right question is whether the likely benefit outweighs the risk for this specific person, at this specific time, in this specific clinical context.
A transparent psychiatrist will discuss issues such as:
- Cognitive impact: whether a medication might cloud attention, slow processing, or create emotional flattening
- Physical tolerability: nausea, restlessness, headache, sedation, or sleep disruption
- Behavioral implications: whether the medication could increase impulsivity, dependence risk, or misuse potential
- Timing: whether a side effect may ease with adaptation or signal the wrong fit entirely
For readers who want a patient-friendly overview of common reactions, understanding medication side effects offers a useful general primer.
Precision matters more in complex cases
One of the clearest examples of clinical precision involves lithium. According to the American Psychiatric Association discussion of complex psychopharmacology, serum lithium levels can become toxic or sub-therapeutic depending on interactions with common diuretics and antihypertensives. That's not a minor technicality. It's a reminder that medication management often requires active coordination between psychiatrists, medical providers, and pharmacists.
Side-effect management isn't a comfort issue alone. It's a safety issue, a performance issue, and a treatment-retention issue.
What doesn't work
In executive care, several approaches reliably fail:
- Prescribing too fast: adding medications before the first one has been properly evaluated
- Ignoring substance use: treating anxiety or insomnia without accounting for alcohol, stimulants, cannabis, or sedatives
- Minimizing complaints: telling a high-functioning patient to “push through” cognitive dulling or fatigue
- Confusing temporary relief with recovery: a medication can reduce acute distress and still be the wrong long-term fit
The most effective medication plans are collaborative. They leave room for frank reporting, timely changes, and the possibility that less medication may be the smarter answer.
Specialized Management for Co-Occurring Disorders
Medication management becomes far more complicated when mental health symptoms and substance use disorder appear together. Anxiety may be trauma-driven, withdrawal-related, or both. Depression may predate the addiction, result from it, or emerge during early abstinence. Sleep disturbance may be a psychiatric symptom, a detox symptom, or a consequence of both.
That's why dual-diagnosis treatment requires a different level of psychiatric discipline. A generic mental health approach can miss the role of substances. A generic addiction approach can miss the psychiatric condition driving relapse.
Where complexity shows up
The central challenge is sorting out what should be treated, what should be observed, and what should be left alone until the clinical picture becomes clearer. That takes time and a team that can tolerate ambiguity without overmedicating it.
Co-occurring disorder management often includes decisions about:
- Withdrawal support: using medication selectively during stabilization without creating new dependence problems
- Relapse prevention: avoiding prescriptions that carry abuse potential when safer options exist
- Polypharmacy control: reducing unnecessary overlap between psychiatric, detox, sleep, and medical medications
- Sequencing: deciding what to address first when several problems are active at once
Why generic advice falls short
Research summarized in this review of treatment barriers for people with co-occurring substance use disorders notes that these patients face unique barriers including stigma and provider shortages. It also highlights the need for a specialized medication optimization approach focused on safety and minimal pharmacology because withdrawal, relapse risk, and polypharmacy create challenges that generic mental health content often overlooks.
For executives and other high-profile professionals, that gap can be especially costly. They're often skilled at compensating, which means they may arrive in treatment with years of partial solutions, layered prescriptions, inconsistent sleep, and substance use hidden under professional success.
In dual diagnosis, the wrong medication can do more than cause side effects. It can confuse the diagnosis, increase relapse risk, and delay real stabilization.
What tends to work better
The most effective psychiatric medication management for co-occurring disorders usually shares several features:
- Fewer moving parts: each medication needs a clear purpose
- Frequent reassessment: symptoms are reviewed as the nervous system settles
- Tight communication: psychiatrists, therapists, and medical staff compare notes instead of working in silos
- Respect for recovery stage: what's appropriate in detox may not be appropriate two weeks later
This approach is especially important in private residential care for professionals. The client isn't only trying to stop using. The client is trying to regain judgment, emotional steadiness, and the capacity to return to a high-accountability life without carrying a chemically overbuilt treatment plan.
Medication Management in a Luxury Executive Program
For executives, environment affects treatment quality more than many people expect. If the setting feels chaotic, exposed, or disconnected from real obligations, even excellent clinical recommendations can be harder to follow. A luxury private-pay residential program solves part of that problem by aligning the clinical process with the client's actual life.
What high-end care should include
A serious executive program doesn't justify its cost with décor alone. It justifies it with structure, staffing, privacy, and access. Real luxury rehab for professionals often means very small programming, private accommodations, and individualized psychiatric attention.
The economics reflect that model. Executive luxury rehab programs can cost over $1,000 per day, with some high-end facilities reaching up to $3,500 daily, according to this overview of executive luxury rehab. In practice, that price point reflects personalized clinical teams and continuous access to advanced care rather than hospitality by itself.
A discreet executive setting should also protect focus. Real private executive rehab programs often keep census small, with eight to twelve people maximum in some programs, which supports confidentiality and reduces the interpersonal volatility that can derail clinical progress.
The executive standard
For working professionals, psychiatric medication management inside residential treatment has to account for real-world demands:
- Electronics access: clients may need appropriate use of phones and laptops to maintain essential career obligations
- Private rooms: sleep, confidentiality, and emotional decompression improve when the living space is fully private
- Integrated care: psychiatrists, psychologists, therapists, and medical staff need shared treatment goals
- Minimal effective pharmacology: medication should support clarity and emotional regulation, not create a sedated version of compliance
One example is licensed psychiatric and psychological staffing in California luxury rehab settings, where clients can receive psychiatric oversight as part of a broader dual-diagnosis model rather than as a disconnected add-on. Reflections is one such California option. It provides psychiatric care, private rooms in detox and rehab, appropriate electronics access for ongoing obligations, and medication optimization within a residential program built for adults who need discretion and high clinical structure.
Why this model fits executives
An executive often enters treatment with two conflicting needs. One is to step back enough to heal. The other is to remain anchored enough that treatment doesn't create fresh professional damage. Luxury residential care can hold both.
That balance is easier when the program is private-pay, clinically dense, and designed for a high-end clientele from the start. The person doesn't need a one-size-fits-all schedule or a crowded setting. The person needs a contained environment where psychiatric decisions are personalized, therapy is intensive, and the treatment plan respects the fact that a serious career is still part of reality.
Frequently Asked Questions and Next Steps
Will treatment remain private
Yes, privacy is a central concern in executive care. Confidentiality matters clinically and professionally. A private room, a small residential setting, and careful communication standards all support that expectation.
Can a client keep working while in treatment
In some executive-focused residential programs, yes. Appropriate access to electronics such as phones and laptops allows clients to stay connected to essential obligations without turning treatment into business as usual. The point is balance, not total immersion in work.
Is medication always part of treatment
No. Some clients need medication. Some need existing medications adjusted or reduced. Some need careful observation before any psychiatric medication is started. The treatment plan should follow the diagnosis and current risks, not habit or convenience.
How long does medication management take
It depends on the clinical picture. Early treatment often involves a trial-and-monitoring period while the psychiatrist tracks benefit, side effects, and stability. In dual-diagnosis care, that timeline can shift as withdrawal resolves and the underlying psychiatric symptoms become clearer.
Are families involved
Often, yes. Family involvement can improve understanding, accountability, and long-term follow-through when it's handled thoughtfully and with the client's consent.
What should happen next
The next step should be simple: a private consultation focused on symptoms, substance use, work demands, current medications, and what kind of residential setting makes sense. For a high-functioning professional, that initial conversation should feel clear, discreet, and specific.
For executives, professionals, and families seeking a confidential path into luxury dual-diagnosis treatment, Reflections offers private-pay residential care in California with psychiatric oversight, medication optimization, private rooms in detox and rehab, and appropriate electronics access to support essential work responsibilities during treatment.









