A decision about treatment often lands in the middle of a live crisis. A founder is missing morning meetings. A physician is charting while withdrawing at night. A partner in a firm is still answering messages, still closing deals, and still telling everyone that things are under control. From the outside, performance may look intact. Inside, concentration is slipping, sleep is fragmented, and the cost of waiting keeps rising.
For high earners and public-facing professionals, the question usually isn't whether help is needed. It's whether treatment can happen without destroying privacy, credibility, and continuity at work. That's why luxury rehab for executives exists as a distinct category. It isn't standard residential care with better sheets and a nicer meal plan. It's a private-pay clinical model built for C-suite leaders, founders, physicians, attorneys, investors, and other working professionals who need serious treatment in a setting that protects both recovery and professional life.
The most important distinction is this. A high-end executive program should be judged less by what it advertises and more by what it makes possible. Can the resident keep a phone and laptop when appropriate? Is there a private room in both detox and residential treatment? Is the clinical team strong enough to treat addiction and co-occurring psychiatric conditions at the same time? Are privacy protocols engineered into daily operations, or are they just promised in admissions calls?
Beyond Amenities Defining True Luxury Executive Rehab
Luxury gets misunderstood in behavioral healthcare. Many people hear the term and think of spa services, chef-prepared meals, or a beautiful property. Those comforts can help, but they're not the reason an executive-level program matters.
For an executive, luxury means functional protection. It means a private room in detox and rehab so sleep can stabilize and confidential calls can happen without exposure. It means a calm environment that lowers stimulation instead of adding to it. It means nutrition that supports cognition and physical recovery rather than treating meals as an afterthought.

What the price is actually buying
The cost of a true executive program is high because the operating model is high-touch. Executive luxury rehab programs typically cost over $1,000 per day, with some high-end facilities reaching up to $3,500 daily, and that pricing reflects personalized clinical teams and continuous access to advanced care rather than décor alone, according to Addiction Resource's overview of executive rehab.
That price point makes sense only when the program delivers a materially different level of service. In practical terms, that usually includes:
- Private accommodations: not upgraded on request, but built into the program as standard.
- Highly credentialed care: access to psychiatrists, PhD-level psychologists, and certified addiction professionals.
- A contained environment: fewer residents, less chaos, and less exposure to the interpersonal volatility that often disrupts early recovery.
- Executive-compatible logistics: space to handle limited work demands without turning treatment into remote office life.
A reader looking at what sets luxury rehab centers apart should pay attention to whether those features are clinical and operational, not just aesthetic.
Practical rule: If a program markets luxury but can't explain how privacy, sleep, nutrition, and individualized psychiatric care improve treatment adherence, it's selling an atmosphere, not a recovery model.
What doesn't work
A glossy setting can hide a weak program. Private-pay clients often enter treatment after months or years of compensating with money, status, and access. If the rehab mirrors that pattern by reducing discomfort without challenging the underlying illness, it won't hold.
The wrong version of luxury indulges avoidance. The right version removes friction so clinical work can happen at full depth. That's the difference.
For executives, the return on investment isn't indulgence. It's restored judgment, emotional regulation, sustained sobriety, and the ability to return to leadership with far more stability than they had when they arrived.
The Clinical Architecture of High-Performance Recovery
High-functioning professionals rarely present with a simple substance problem. They arrive with layered symptoms. Alcohol may be managing social anxiety. Stimulants may be covering depression and exhaustion. Sedatives may be compensating for trauma-related insomnia. If treatment addresses only the substance, the system underneath remains unchanged.
That's why the core of luxury rehab for executives should be dual-diagnosis care. The clinical architecture needs to treat substance use and mental health conditions simultaneously, not sequentially.
Why dual diagnosis isn't optional
The clinical architecture of executive luxury rehab is defined by a dual-diagnosis integration model that treats substance use disorders and co-occurring mental health conditions simultaneously. Evidence from the American Society of Addiction Medicine indicates that this approach reduces the 12-month relapse rate by 35% compared to SUD-only treatment.
That single fact changes how a serious program should be evaluated. A resident with trauma, panic, bipolar symptoms, depression, or chronic grief won't stay well for long if those conditions are left untreated. Sobriety without psychiatric stabilization often becomes a short-term interruption, not recovery.
A strong personalized treatment planning process should identify those drivers early and build treatment around them instead of adding them later as secondary concerns.
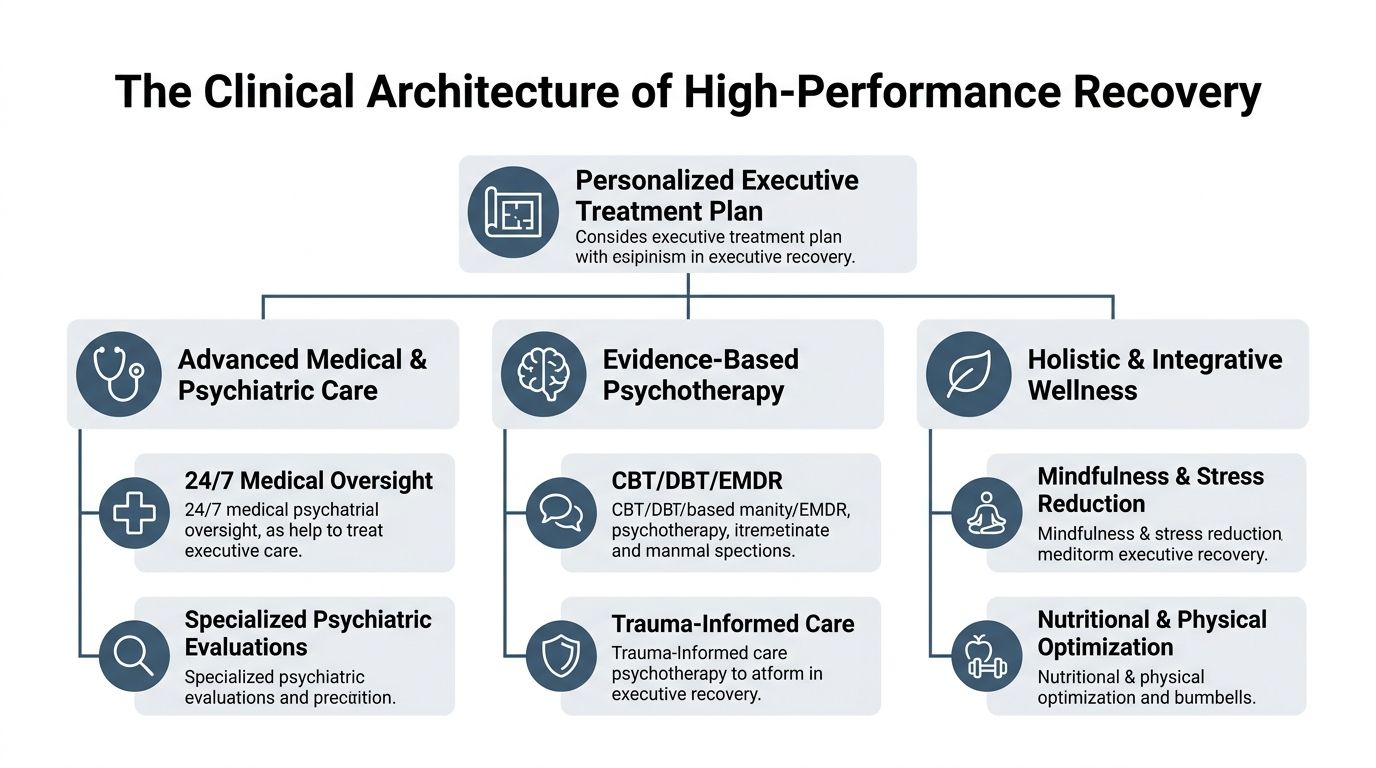
What the treatment plan should include
The best executive programs combine medical, psychotherapeutic, and somatic interventions. Not every resident needs every modality, but the program should be able to deploy them as the clinical picture evolves.
A high-caliber plan often includes:
- Medical and psychiatric assessment: medication review, withdrawal management, sleep stabilization, and diagnostic clarification.
- Evidence-based psychotherapy: CBT, DBT, ACT, motivational work, trauma-focused therapy, and carefully structured individual sessions.
- Experiential and nervous-system regulation work: mindfulness, art-based therapies, equine work, movement, and somatic interventions that help residents shift out of chronic hyperarousal.
- Advanced options where appropriate: some executive programs also use tools such as TMS or EEG neurofeedback to support regulation, attention, and mood stability.
A resident may look productive in the outside world and still be clinically exhausted, dissociated, or severely anxious. Good treatment doesn't reward that mask. It assesses what's underneath it.
Why individualized intensity matters
Executives often need fewer performative groups and more clinically targeted contact. The work has to be direct. It should identify defensive patterns, perfectionism, control needs, shame, family-of-origin dynamics, and the way success has been used to outrun distress.
Programs that rely heavily on generic group schedules usually miss the mark with this population. The more effective model uses individual therapy to translate insight into immediate behavior change. That includes how the resident handles stress, boundaries, sleep, work urgency, relationships, and relapse risk.
In practice, the aim isn't merely abstinence. It's a durable return of executive function in the true sense of the term: better judgment, better impulse control, better emotional tolerance, and less dependence on substances to get through the day.
Maintaining Professional Momentum During Treatment
Executives often ask the wrong first question. They ask whether they'll be allowed to keep their phone. The more important question is whether the program knows how to contain work so it doesn't consume treatment.
The answer shouldn't be blanket prohibition or unrestricted access. It should be structure.
Electronics are useful, but only inside a clinical frame
Top-tier executive rehab facilities explicitly maintain policies that allow residents to retain personal electronics, including cell phones and laptops, to facilitate continued engagement with career obligations, a defining feature of programs built for working professionals, as outlined in this executive rehab resource.
That policy matters. For C-suite leaders and owners, complete digital isolation may be unrealistic. Time-sensitive approvals, legal decisions, payroll issues, investor communication, and succession planning don't always stop because treatment begins.
But access alone isn't a treatment model.
What a workable structure looks like
A serious executive program usually builds work into the day in a narrow, supervised way. That often means:
- Protected clinical hours when therapy, psychiatric care, groups, and recovery tasks come first.
- Limited business windows for urgent communications, not open-ended workdays.
- Private workspace options so calls don't compromise confidentiality.
- Staff collaboration around what's necessary, what can wait, and what should be delegated.
Executives who are used to white-knuckling through fatigue often need explicit permission to stop operating at full output. That's especially important in early stabilization, when concentration and decision-making may be impaired.
For professionals trying to rebuild focus in a healthier way, resources on how to enhance mental clarity for professionals can be useful as part of a broader discussion about sleep, nutrition, and cognitive recovery. They shouldn't replace treatment, but they can support better work habits after the acute phase.
Clinical boundary: If work activity raises anxiety, fragments attention, or becomes a way to avoid treatment, it isn't helping continuity. It's delaying recovery.
A program built around working from rehab should make that distinction clearly. The resident doesn't need to disappear professionally, but neither should treatment become a disguised executive suite with therapy added around the edges.
The right balance preserves momentum where it matters. Board-level essentials get handled. Reputation stays intact. Recovery remains the primary job.
How to Vet a Program for Uncompromising Privacy
Privacy claims in luxury treatment are often too vague to trust. “Discreet,” “confidential,” and “exclusive” sound reassuring, but they don't describe an operating system. Executives need more than a promise. They need to know how confidentiality is protected from first contact through discharge.
The risk isn't always clinical staff. In high-end settings, exposure often happens through ordinary operational gaps. Front desk conversations. Driver coordination. Housekeeping familiarity. Casual staff culture. Those details matter because high-profile residents are easier to identify and more costly to expose.
Ask operational questions, not branding questions
A 2024 investigation by the Journal of Health Privacy revealed that luxury rehabs can have a higher rate of unintended disclosure due to their resort-like culture. True privacy requires privacy-by-design protocols, including mandatory NDAs for all non-clinical employees and encrypted communication channels.
That should change how an executive evaluates any facility. Instead of asking whether the program is private, ask how privacy is engineered.
Use questions like these:
- Who signs confidentiality agreements: only licensed staff, or every employee and contractor?
- How are calls and messages handled: through encrypted systems, or through ordinary front-office processes?
- How does admission work: standard intake traffic, or a controlled process that minimizes visibility?
- Who can see identifying information: everyone involved in operations, or only essential personnel?
Verify the outer perimeter too
A strong facility will secure internal operations. High-profile clients may also want to think about personal device security, office exposure, and travel vulnerabilities before admission. For that reason, information about TSCM bug sweeping services can be relevant in especially sensitive situations involving public figures, litigation, or corporate control issues.
Privacy isn't a hospitality feature. It's a risk-management discipline.
Programs that treat confidentiality as branding usually speak in generalities. Programs that take it seriously can describe process. They'll explain staff training, restricted information flow, secure communications, private admissions, and how they handle visitors, packages, transportation, and schedule exposure.
An executive doesn't need a sales pitch here. A clear answer is enough. If the answer stays vague, that's the answer.
A Framework for Evaluating Executive Rehab Programs
At this stage, the question is no longer whether a program looks private or comfortable. The question is whether it can treat a high-functioning, high-responsibility adult without letting image outrun clinical substance.
I advise families to screen executive programs across four areas: oversight, staffing, treatment fit, and discharge discipline. That framework gets past marketing language quickly.
Accreditation and governance
Begin with licensure and recognized accreditation. Those are baseline protections, not proof of superior care. They show that the facility is subject to external standards, formal review, and corrective accountability.
Then examine governance. Ask who holds final clinical authority, how often cases are reviewed, and how psychiatry, primary therapy, and addiction treatment are coordinated when the resident is under strain. Executives often enter treatment after a long period of compensating. A weak chain of command tends to show up when sleep collapses, irritability rises, or work pressure starts pulling attention away from treatment.
Clear answers matter here. Vague answers usually mean diffuse responsibility.
Team credentials and staffing depth
The next issue is staffing depth, not staffing theater. A website may list impressive titles, but the operative question is who sees the patient, how often, and with what level of authority.
Ask specifically:
- Who owns the case: a senior licensed clinician, or an admissions-facing coordinator passing updates between departments?
- Who manages psychiatric care: an on-site psychiatrist with regular follow-up, or a consultant with limited contact?
- Who treats trauma, mood symptoms, and substance use together: one integrated team, or separate tracks that do not communicate well?
- Who works with the family: a designated clinician, or whoever has time that week?
Reflections describes a California-licensed, Joint Commission-accredited dual-diagnosis model with private accommodations, clinically managed detox, and appropriate electronics access for working professionals. That description is useful because it tells you how care is structured, not just how the property photographs.
Treatment design and fit
Treatment design decides whether an executive can stabilize or white-knuckle the stay. The right program should be able to explain what happens when a resident is guarded, sleep-deprived, accustomed to control, and still trying to manage business problems from inside treatment.
Use a practical screen:
| Evaluation area | What to ask |
|---|---|
| Dual diagnosis | How are psychiatric symptoms and substance use treated in one coordinated plan? |
| Individualization | How much direct one-to-one work is built in, and what determines that level of intensity? |
| Executive compatibility | How is work access handled without letting email, calls, and deal pressure derail treatment? |
| Detox continuity | If detox is needed, how does the clinical approach carry forward into residential care? |
One trade-off deserves direct attention. Programs that allow unrestricted device use may preserve short-term business continuity, but they often prolong avoidance and keep the nervous system in a constant state of activation. Programs that ban all access can create a different problem if the client holds material decision-making authority. The better model is structured access with clinical boundaries, planned windows, and staff who know when work is supporting stability and when it is functioning as an escape.
Outcome measurement and aftercare discipline
A strong program can explain how it measures progress during treatment and how it decides that a resident is ready to step down. The answer should cover engagement in therapy, psychiatric stabilization, relapse risk, family participation, work re-entry planning, and the continuing-care structure after discharge.
Be cautious if the admissions conversation keeps returning to chef-prepared meals, scenic grounds, or comfort features without equal fluency on clinical process. That usually signals an imbalance. Residential treatment can create a period of safety and momentum, but it cannot carry recovery alone. Executives tend to do best when discharge planning is as deliberate as admission, with a realistic schedule for therapy, medication follow-up, family work, accountability, and the return of professional responsibilities.
A polished setting can help. It cannot compensate for a thin clinical spine.
The Executive Journey From Admission to Aftercare
The treatment course for an executive should feel contained, private, and clinically coherent from the first call forward. Most stays run 30 to 90 days, and the strongest programs match length of stay to psychiatric complexity, relapse history, medical needs, and how stable the home and work environment will be after discharge.
The first phase is admission and assessment. Contact should be confidential, efficient, and low exposure. Once admitted, the resident moves into a private room, often beginning with detox if needed. For high-functioning professionals, private accommodations matter immediately. They reduce stimulation, protect sleep, and give the nervous system room to settle.
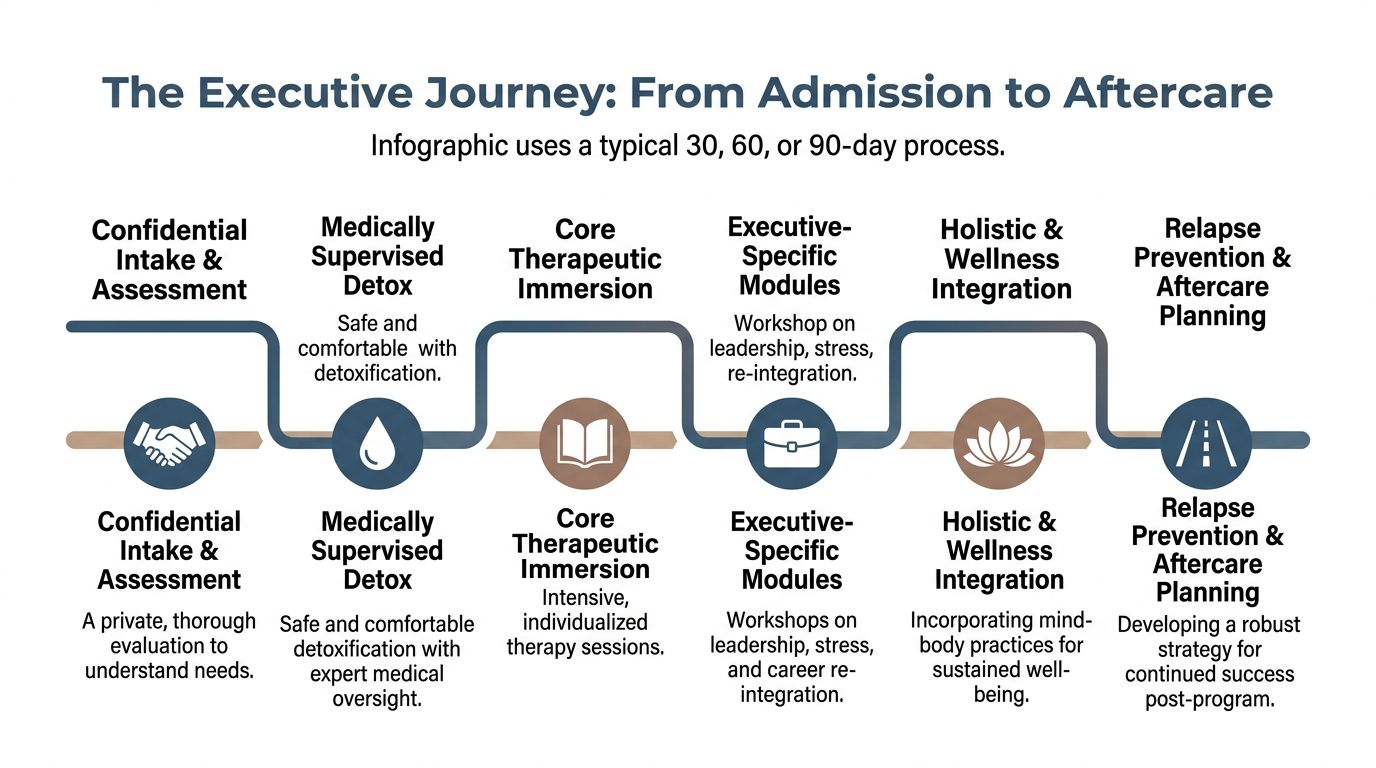
What the residential day often includes
A representative day in executive treatment is structured, but it shouldn't feel chaotic or overpacked. The rhythm usually includes psychiatric follow-up, individual therapy, focused group work, wellness activity, meals designed to support recovery, and a limited work window if clinically appropriate.
What matters is intensity. Top executive programs maintain a high clinician-to-client ratio, such as 1:3 or 1:4, which is linked to lower dropout rates and stronger outcomes. Programs also track return-to-work metrics, with successful models showing 75% of executives returning to their roles within 6 months post-discharge.
That level of staffing changes the experience. Residents are less likely to disappear into the program anonymously. Patterns get noticed quickly. Avoidance gets addressed early. Treatment can adapt in real time when a client destabilizes, withdraws, or starts over-functioning.
The return home is part of treatment
Residential care is only one part of the arc. Executives often relapse or decompensate after discharge not because treatment failed, but because the re-entry plan was thin. The inbox returns. Travel resumes. Relationship strain reappears. Old coping patterns get reactivated.
A strong aftercare plan usually includes:
- Clinical continuation: therapy, psychiatry, and medication follow-up where appropriate.
- Relapse prevention mapping: concrete planning around travel, alcohol-centered work events, fatigue, and high-risk relationships.
- Family involvement: expectations, boundaries, and education for the home system.
- Professional reintegration: a realistic strategy for workload, delegation, and gradual return to full intensity.
The discharge date shouldn't mark the end of structure. It should mark the transfer of structure into real life.
For executives, sustained recovery depends on whether treatment prepared them for the environment they're returning to. The best programs know that and plan accordingly.
Your Checklist for Making an Informed Decision
A busy executive or family member doesn't need more marketing language. They need a short list that exposes whether a program is built for serious, private, high-end treatment. The easiest way to compare options is to score each one against the same operational questions.
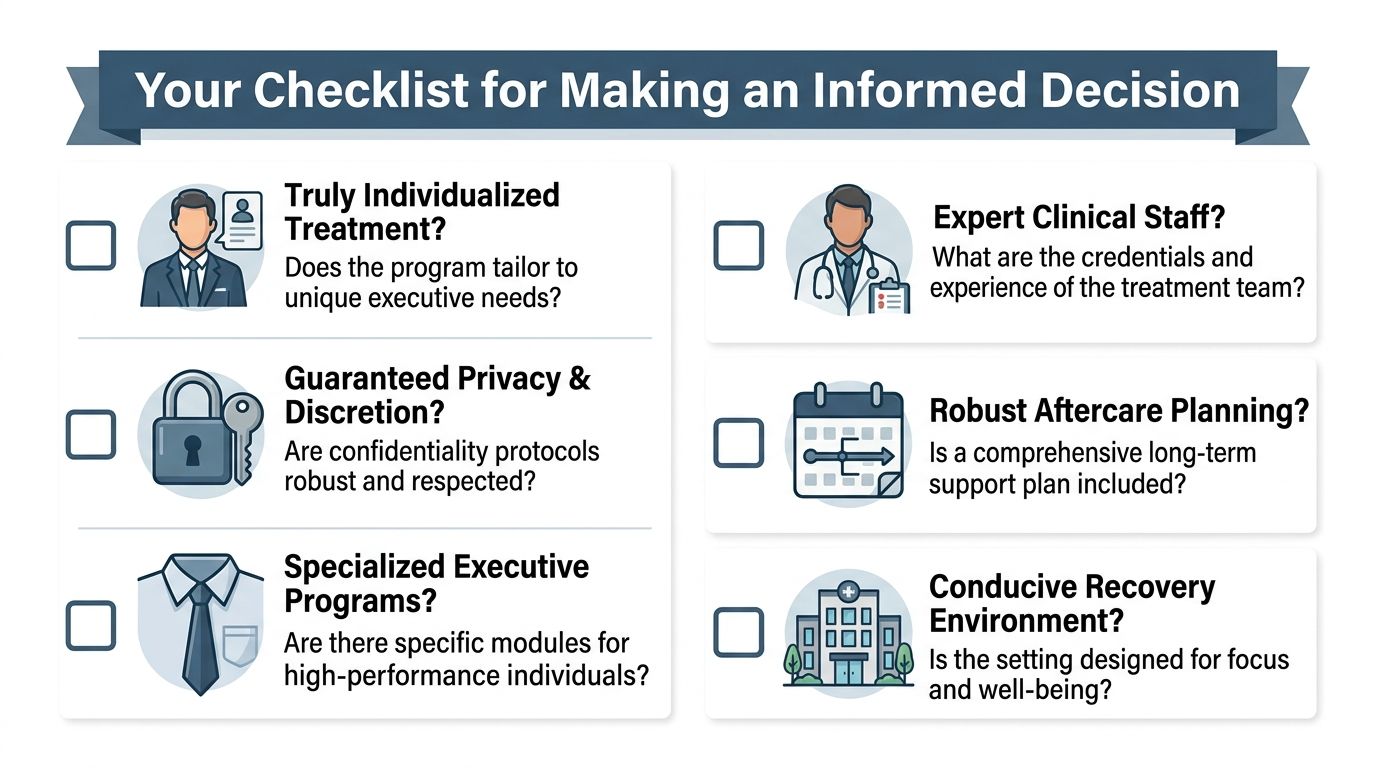
Clinical quality checklist
Use this first group to determine whether the program is medically and psychologically credible.
- Dual-diagnosis treatment is central: substance use and mental health are treated in one integrated plan.
- Private rooms are standard: both detox and rehab protect sleep, privacy, and dignity.
- The clinical team is highly credentialed: psychiatry, licensed therapists, addiction specialists, and senior oversight are clearly defined.
- Treatment includes evidence-based modalities: CBT, DBT, ACT, trauma-informed work, and individualized psychotherapy are available.
- Medication strategy is thoughtful: withdrawal management and psychiatric care are available without turning treatment into medication-only stabilization.
Executive-fit checklist
This group separates general luxury care from true luxury rehab for executives.
- Electronics policy is explicit: residents may keep cell phones and laptops when clinically appropriate.
- Work access is structured: there are private spaces and defined boundaries around business continuity.
- The program understands high-performance psychology: control, overwork, shame, perfectionism, and image management are addressed directly.
- The environment supports cognitive recovery: quiet, order, nutrition, sleep protection, and low interpersonal chaos are part of the design.
Privacy and discharge checklist
The final screen is often the deciding one.
- Privacy-by-design protocols are in place: NDAs cover non-clinical staff, communications are secure, and admissions are discreet.
- Information flow is restricted: not every employee can access identifying details.
- Aftercare is specific: the program can explain what support follows residential treatment.
- Return-to-work planning is realistic: the resident leaves with a strategy for travel, stress, social exposure, and workload.
- Family or key stakeholders can be involved appropriately: not by default, but with clear therapeutic purpose and consent.
A final test helps when everything looks polished. Ask the admissions team to walk through an actual executive case in anonymous terms. How would they handle detox, work demands, privacy risks, psychiatric complexity, and re-entry? Strong programs answer with process. Weak ones answer with adjectives.
Luxury treatment is worth its cost only when it protects what matters most. Health, privacy, and the ability to return to professional life with more stability than before.
Reflections provides private-pay, luxury dual-diagnosis treatment for executives, C-suite leaders, and working professionals who need confidential residential care without abandoning important career responsibilities. With private rooms in detox and rehab, a highly accredited clinical team, and appropriate access to electronics for business continuity, Reflections offers a discreet path for adults who need high-end treatment grounded in serious clinical work.









