A private equity partner is still replying to board messages at midnight. A founder is drinking alone after investor calls. A physician executive is hiding withdrawal symptoms behind a polished calendar and a calm voice. On paper, nothing looks broken. Revenue is up. The team is intact. The family may even believe things are manageable.
But high performers often wait too long because they assume treatment requires professional disappearance. They picture locked schedules, shared rooms, confiscated devices, and a public unraveling of the identity they've spent years protecting. That fear keeps many executives stuck.
A more refined model exists. In the right setting, work from rehab can be integrated into treatment without turning rehab into an office. The distinction matters. Recovery doesn't improve because someone keeps answering email. It improves when clinical care stays protected, stress is managed, and work is used carefully instead of compulsively.
For high-achieving professionals, that balance has to be built with precision. Privacy must be real. Clinical oversight must be strong. Device access must be structured. The goal isn't to preserve the old pace that helped create the crisis. The goal is to maintain necessary career continuity while repairing the health, judgment, and emotional stability that make leadership sustainable.
The Executive's Dilemma Healing Without Halting Your Career
At 6:15 a.m., a CEO joins a strategy call from a guest room, camera on, voice steady, while privately wondering whether tremors will start before lunch. By evening, that same person may still be approving budgets, answering investors, and telling family everything is under control. This is how the dilemma usually presents. Performance remains visible. The cost stays hidden.

For senior professionals, the central question is rarely whether work matters. It does. The primary question is whether work can be contained well enough that treatment still does its job.
I tell clients to judge the situation by risk, not pride. If substance use, insomnia, panic, depression, or burnout have started to impair judgment, memory, emotional control, or physical stability, continuing at full speed is not career protection. It is exposure. The immediate fear is stepping away. The larger threat is staying in role while functioning deteriorates behind the scenes.
Why the fear feels rational
Executives often carry obligations that do not pause cleanly. They may control key client relationships, hold signing authority, supervise regulated functions, or serve as the public face of a company during a sensitive period. Many also understand, correctly, that colleagues can be sympathetic about stress and far less informed about addiction, trauma, or co-occurring psychiatric care.
That makes hesitation understandable.
What often helps is a shift in frame. Treatment does not need to mean disappearing from professional life entirely. In a properly designed setting, work can be treated as one part of the care plan to manage carefully, much like sleep, medication timing, family communication, and exposure to stress. The point is not to preserve the habits that helped create the crisis. The point is to keep only the responsibilities that are genuinely time-sensitive, while restoring the judgment and stability that make work sustainable.
What high performers often get wrong
Many accomplished people ask whether they can keep working in rehab. A better question is how much work their clinical team believes they can handle without disrupting detox, therapy, psychiatric care, and recovery momentum.
That distinction matters. I have seen limited work access help a client stay calm, protect a transition, or prevent unnecessary business fallout. I have also seen work used as avoidance. Constant emailing, compulsive monitoring, and taking calls during emotional strain can keep the nervous system in the same state that fueled the problem outside treatment.
A work-friendly luxury rehab for tech executives in Silicon Valley should account for that trade-off directly. The setting matters, but the clinical boundaries matter more.
What a modern luxury model gets right
A strong luxury program gives clients privacy, discretion, and enough flexibility to protect legitimate business obligations. It also sets limits. Work happens in planned windows. Therapy remains protected. Medical needs take priority. Staff monitor whether professional contact is supporting stability or feeding the same cycle of pressure, control, and emotional escape.
The model is more elaborate than simple permission to bring a laptop. Work is not treated as a perk. It is integrated carefully, with clinical oversight, because for some clients the healthier goal is not withdrawal from career identity forever. It is rebuilding a different relationship with ambition, availability, and stress.
That change often becomes one of the most valuable parts of treatment. Clients do not just keep the lights on at work. They learn how to return with better boundaries, clearer thinking, and a reduced need to use achievement as cover for distress.
Choosing a Truly Work-Compatible Luxury Rehab
Many facilities say clients can bring a laptop. That detail alone means very little. For an executive, work-compatible treatment isn't about permission. It's about whether the environment can support confidential, bounded work access without undermining clinical intensity.
A serious program is designed around containment. That means a private room for calls, protected therapy hours, a staff culture that understands executive psychology, and a schedule where work must fit inside treatment rather than compete with it. For professionals evaluating options, a useful reference point is this overview of a work-friendly luxury rehab for tech executives in Silicon Valley.
The difference between access and structure
Some clients hear “electronics allowed” and assume they can continue business as usual. That assumption usually backfires. Unrestricted access invites the same habits that drove dysregulation outside treatment, including compulsive checking, avoidance through busyness, and the inability to tolerate emotional discomfort without distraction.
What works better is a controlled model.
| What to look for | Why it matters |
|---|---|
| Private accommodations | Confidential calls, document review, and decompression require physical privacy |
| Protected treatment blocks | Therapy can't become the thing that gets moved whenever a message arrives |
| Clinically supervised device access | Staff need to notice when work is becoming an avoidance strategy |
| Executive-calibrated communication | Sophisticated clients respond better to direct, non-punitive boundary setting |
| Quiet, secure infrastructure | Sensitive work requires more than guest Wi-Fi and a shared lounge |
Questions worth asking before admission
A high-performing client should ask practical questions, not marketing questions.
- Where will calls happen? A private room is very different from “quiet space available.”
- Who decides when work access is appropriate? The answer should involve clinical judgment, not convenience.
- How is detox handled? Early stabilization often changes what a client can realistically manage.
- What happens if work begins interfering with care? A credible program will have a process for recalibrating access.
- How are co-occurring symptoms treated? Executives often present with anxiety, depression, trauma, or bipolar-spectrum symptoms that directly affect work capacity.
A luxury environment should reduce friction around recovery. It should not increase a client's ability to hide from treatment in comfort.
Ethics matter as much as amenities
There's another line discerning clients should understand clearly. Voluntary remote-work access is not the same as being required to work in treatment. A 2024 investigative report found some facilities were requiring unpaid work from patients. Ethical high-end programs draw a hard distinction between supporting access to a client's own career and imposing labor as part of treatment (investigative reporting on coercive work practices in rehab).
That ethical line matters because executives are often used to high demands and may minimize exploitation if it's framed as discipline or accountability. In quality care, work remains the client's choice, tightly bounded, and secondary to treatment.
What doesn't work
The wrong setup usually fails in predictable ways:
- Shared living with no acoustic privacy. Confidentiality disappears.
- Ad hoc device access. The day gets fragmented and therapy attendance slips.
- A hospitality-only model. Luxury without clinical rigor leaves the core problem untouched.
- Staff who romanticize hustle. Professionals don't need praise for overfunctioning. They need help interrupting it.
For executives, the right rehab isn't just work-friendly. It's clinically protective, discreet, and operationally realistic.
Navigating Workplace Communication and Medical Leave
A client can handle detox, assessment, and the emotional weight of admission, then still lose sleep over one email to HR.
For high-performing professionals, workplace communication is often the most charged part of the process. The risk is not only saying too much. It is also creating loose expectations that pull work back into treatment before the clinical team has set safe limits. In a well-run luxury program, communication is part of treatment planning because it affects stress load, availability, and the client's ability to separate urgent from merely important.
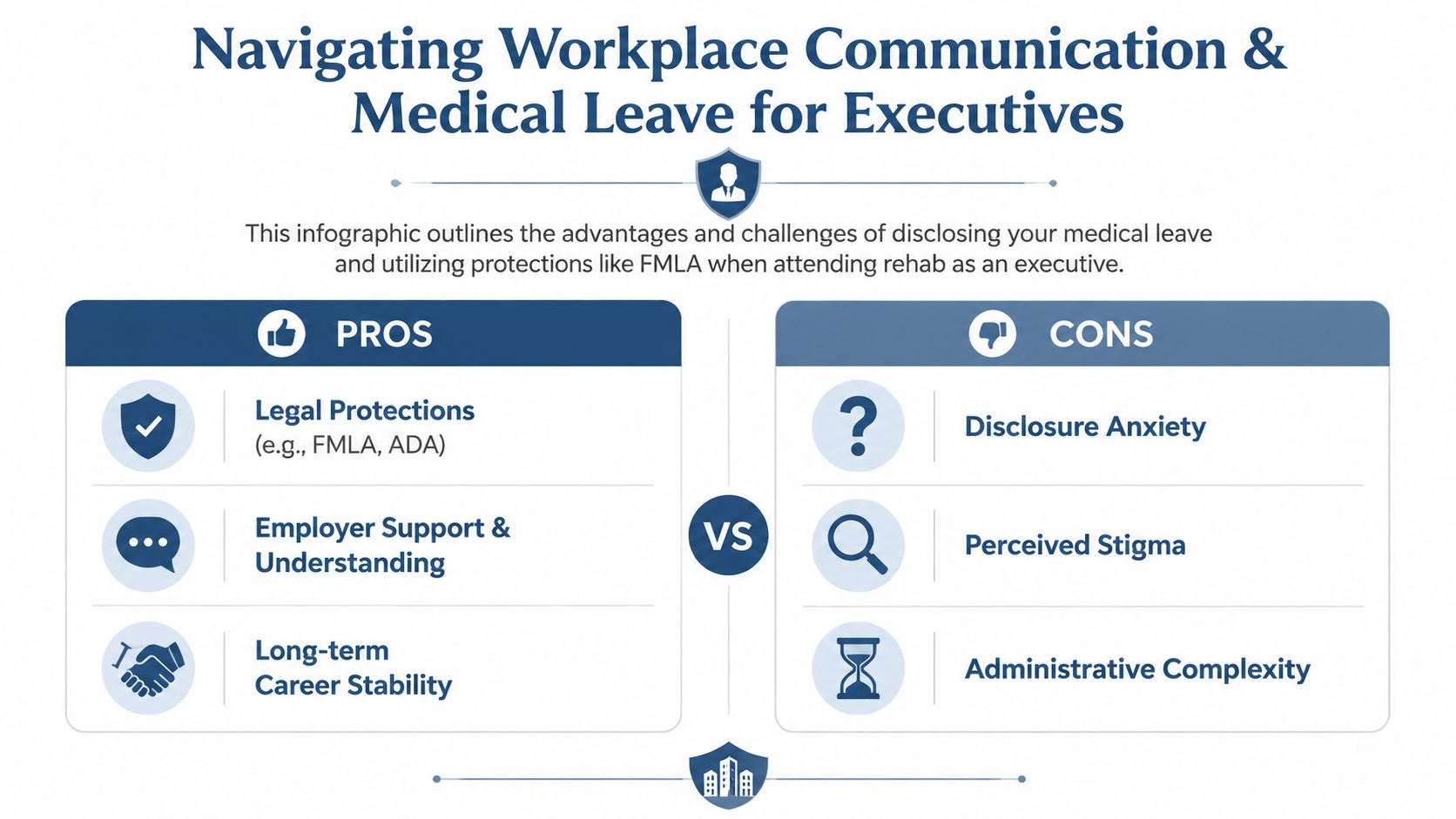
The goal is simple. Protect privacy, preserve professional standing, and keep the leave structure tight enough that recovery remains the primary job.
Keep the message clinical and brief
Treatment is healthcare. The language should reflect that.
In practice, executives usually need two versions of the same message. One goes to HR, legal, or whoever handles leave administration. That version should confirm that a medical condition requires treatment, that leave needs to be documented, and that future communication should stay limited to administrative needs. The second version goes to colleagues, clients, or direct reports who only need continuity information. That message should cover timing, interim coverage, and the point person for urgent matters.
A useful operational reference is this complete guide for modern workplaces, especially if you need to understand how employers typically define and process a leave of absence.
Set boundaries before admission
This is the part many professionals mishandle. They announce a leave, then offer assurances they will still be available for strategy calls, approvals, or late-night problem solving. That arrangement usually creates confusion on both sides. The company hears access. The treatment team sees divided attention. The client ends up trying to satisfy both.
A better plan sets the boundary first. If limited work contact may continue later, say that any availability will depend on medical guidance and treatment progress. That protects the client from making promises in a pre-admission panic and gives the clinical team room to decide whether work can be integrated safely.
“I am taking medical leave for treatment. For business continuity, please route urgent matters to the designated contact while I am away.”
Use a controlled communication sequence
The cleanest leave conversations follow a narrow path:
- Choose one primary decision-maker. That may be HR, a managing partner, general counsel, or a direct supervisor.
- Separate health disclosure from operational planning. Medical information stays limited. Coverage planning gets its own conversation.
- Assign one internal point person. This reduces pressure to monitor every message personally.
- Confirm the basics in writing. Leave dates, benefits questions, and emergency contact expectations should not live in verbal side conversations.
- Review any planned work contact with the treatment team. In some cases, a small amount of structured communication supports stability. In other cases, it keeps the client psychologically fused to the job.
That last point matters. In a luxury setting, work access should serve the recovery plan, not the other way around.
Decide who actually needs to know
Broad disclosure rarely helps. In many workplaces, “medical leave” is sufficient. Senior professionals often assume they owe a full explanation because they are visible, responsible for revenue, or accustomed to answering every question. They usually do not.
Selective disclosure protects dignity and reduces gossip. It also lowers the chance that coworkers start treating treatment as a public narrative instead of a private health matter. If a client chooses to share more with a trusted founder, board chair, or partner, that choice should be deliberate and limited, not emotional and improvised.
For more detailed guidance on language and timing, this resource on how to talk to your employer about going to rehab can help shape the conversation before leave begins.
The standard I recommend is proportion. Say enough to secure lawful leave, establish business continuity, and protect your reputation. Say little enough that treatment can begin without turning your private medical care into workplace content.
Structuring Your Day for Recovery and Productivity
The best work-from-rehab schedule looks boring on purpose. It has clear treatment blocks, limited work windows, protected meals, rest, movement, and transition time. That predictability is what keeps work from spreading across the entire day.
A common mistake is assuming remote access equals normal capacity. It doesn't. Early treatment often involves withdrawal management, psychiatric evaluation, medication adjustments, emotional volatility, and cognitive fatigue. The client who insists on handling negotiations from day three is usually trying to preserve identity, not make a sound clinical decision.
The first phase should feel narrower
Programs that protect outcomes tend to preserve treatment dose. One practical benchmark from treatment reporting is that completion matters greatly, yet only about 45% of people in long-term residential treatment finish their programs. The same treatment summaries note that programs lasting 90 days or more consistently show better outcomes, which is why managed work access needs to support retention instead of competing with it.
In practical terms, the first stage of rehab should be clinically heavy and professionally light. That usually means no discretionary meetings, no constant messaging, and no emotionally loaded business decisions unless there is a genuine necessity.
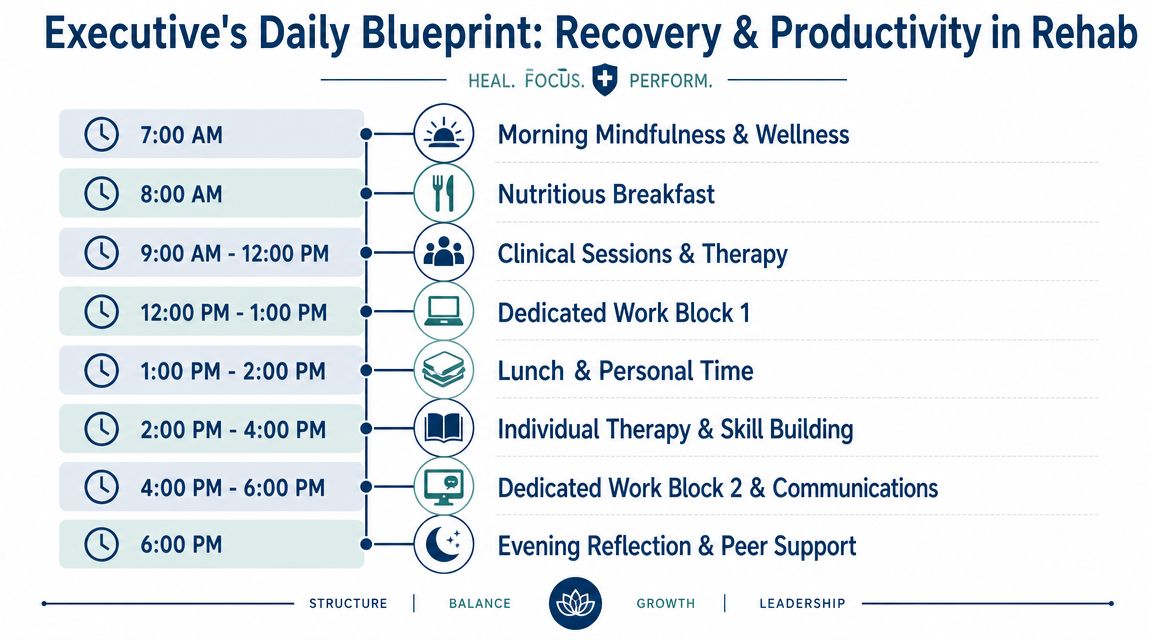
A workable daily rhythm
A strong executive schedule usually follows a pattern like this:
- Morning belongs to treatment. Individual therapy, group work, psychiatric follow-up, and recovery assignments happen before the nervous system is depleted by business demands.
- Midday work is brief and pre-planned. One focused block is enough for urgent email review, delegated approvals, or a short leadership check-in.
- Afternoon returns to clinical work. Trauma treatment, skills practice, family sessions, and dual-diagnosis care need alert attention.
- Evening is for downshifting. Reflection, peer support, movement, and sleep preparation matter more than squeezing in one more conference call.
Operational test: If a work task leaves a client too activated, distracted, or depleted to participate fully in therapy afterward, that task is too heavy for residential treatment.
Which work tasks fit and which do not
Not all work is equally disruptive. The safest tasks are usually contained, predictable, and low in emotional volatility.
| Better fit during rehab | Poor fit during rehab |
|---|---|
| Approvals with clear boundaries | Crisis negotiations |
| Short team updates | Personnel conflicts |
| Document review | High-stakes investor or litigation strategy calls |
| Delegation and transition planning | Tasks that trigger perfectionism and control spirals |
| Limited email triage | Open-ended inbox monitoring all day |
The goal is to preserve continuity, not dominance. A client may stay connected without remaining central.
Boundaries that keep the plan intact
The schedule works only if the workplace understands it. Executives should set response windows, designate a backup contact, and tell key stakeholders that silence during treatment blocks is expected, not alarming.
A few rules help:
- Use scheduled communication windows. Colleagues adapt quickly when they know when replies will come.
- Avoid reactive log-ins. Every “just checking” moment can become an hour of dysregulation.
- Protect post-session time. Therapy often surfaces grief, shame, anger, or trauma. Jumping straight into business can shut the process down.
- Review work access weekly. Capacity changes. What's manageable in week three may not have been safe in detox.
Some clients worry that structure is restrictive. In treatment, structure is what creates enough stability for both healing and competent professional functioning. Without it, work expands, recovery contracts, and both suffer.
Ensuring Security and Confidentiality While Working Remotely
For a senior professional, privacy concerns aren't cosmetic. They may be dealing with confidential patient records, privileged legal information, acquisition materials, personnel matters, or market-sensitive conversations. If a treatment setting can't protect discretion, work from rehab becomes unworkable no matter how attractive the residence looks.
The most important question isn't whether a facility has internet. It's whether the environment supports secure, private remote engagement. A useful parallel comes from telerehabilitation research in another clinical field, where successful remote participation depended heavily on support, access, and technology readiness. For executives in treatment, the same logic applies. Success depends on a private setting and secure infrastructure, not simple connectivity (telerehabilitation findings on support and technology access).
What a secure setup includes
A professional-grade setup is built from several layers working together.
- Private physical space. A personal room with a door is the starting point for calls, document handling, and screen privacy.
- Hardened devices. Laptops and phones should be encrypted, password-protected, and configured to lock quickly when unattended.
- Secure network practices. Sensitive conversations and file access should happen through approved company security protocols, not casual consumer shortcuts.
- Limited paper exposure. Printed material creates avoidable risk inside any residential environment.
For healthcare leaders and anyone handling regulated information, security expectations should be explicit. This overview of securing patient data with HIPAA penetration tests is a useful reminder that strong privacy protection depends on systems, testing, and disciplined processes, not assumptions.
Clinical privacy and business privacy are different
Many executives blur these together. Clinical confidentiality protects treatment information. Business confidentiality protects employer or client information. Both matter, but they require different habits.
A facility can support treatment privacy through discreet operations, private accommodations, and controlled communication. The client still has to protect business materials through careful device use, document handling, and call discipline. For readers evaluating standards around protected health information in a treatment environment, this resource on HIPAA compliance in rehab settings can help clarify the basics.
The safest arrangement is simple. Handle sensitive work only in a private room, on secured devices, during planned windows, and only when the task genuinely needs personal attention.
Common failures to avoid
Security problems usually come from convenience. A client takes a call on speaker. A confidential slide deck stays open during a therapy transition. A borrowed charger leads to device wandering. A room door is left unsecured during dinner.
None of this is dramatic. It's just preventable. High-achieving clients often focus on whether they can keep working. The better discipline is deciding how little access is necessary to keep responsibilities covered without exposing confidential information or destabilizing treatment.
Planning Your Aftercare for a Sustainable Return to Work
Residential treatment is a protected environment. Calendars are structured. stressors are reduced. Clinical support is close. The ultimate test comes after discharge, when the old inbox, old relationships, old expectations, and old rewards return all at once.
That's why aftercare can't be an afterthought. It is the bridge between progress inside treatment and durable functioning outside it. Treatment reporting cited in rehab outcome summaries notes that among patients who complete their programs, roughly 69% remain sober at six months, which is one reason a strong aftercare plan matters so much after discharge.
What a serious aftercare plan includes
A high-functioning professional needs more than a list of referrals. The plan should answer how work pressure will be handled when the protective structure is gone.
Core elements usually include:
- Individual therapy with continuity. The therapist should understand both addiction and the executive environment.
- Psychiatric follow-up when indicated. Medication changes made in treatment need monitoring.
- Recovery community connection. Alumni programming, peer accountability, or other support structures help reduce isolation.
- Family involvement. Home patterns often need as much repair as work patterns.
- A written work reentry plan. This should cover travel, events with alcohol, late-night communication habits, and escalation triggers.
The return-to-work questions that matter
Before discharge, the client should be able to answer a few hard questions clearly.
| Question | Why it matters |
|---|---|
| What situations at work most reliably destabilize mood or cravings? | Triggers are easier to manage when they're named in advance |
| Who knows enough to help if work starts replacing recovery again? | Isolation is risky for high performers |
| What boundaries will be visible on the calendar? | Unscheduled ambition quickly fills open space |
| What is the plan after a bad day, not just a good week? | Recovery durability shows up under stress |
A sustainable return to work is not a return to the exact conditions that made treatment necessary.
Protecting the investment
Many executives leave residential care feeling physically better and mentally sharper. That improvement can create false confidence. They want to make up for lost time, clean up every backlog, and prove nothing has changed. In reality, something should change. A healthier schedule, fewer secrecy habits, less emotional self-medication, and better delegation are signs of progress, not compromise.
Aftercare works best when it treats ambition as something to channel, not suppress. The executive doesn't need a smaller life. The executive needs a life that no longer depends on exhaustion, substances, or untreated psychiatric strain to remain productive.
Reflections offers confidential, private-pay luxury treatment for executives, founders, physicians, attorneys, and other high-achieving professionals who need serious dual-diagnosis care without abandoning every career responsibility. With private rooms, appropriate access to electronics, sub-acute detox, evidence-based therapy, and continuing care designed for real-world reentry, Reflections helps clients stabilize, protect their privacy, and build a version of success that recovery can sustain.









