A senior executive can look composed in every meeting, deliver under pressure, and still feel privately controlled by alcohol, stimulants, prescription medication, or another compulsive pattern. That split is common in high-functioning addiction. Outward performance stays intact longer than many people expect. Internally, sleep worsens, stress tolerance narrows, and old trauma starts shaping decisions in ways that feel irrational but hard to stop.
For many professionals, addiction isn't merely a matter of poor discipline. It's often tied to a nervous system that learned to survive overwhelming experiences by staying hyper-alert, emotionally shut down, or chronically soothed by substances. When that's the pattern, treatment has to reach deeper than surface behavior.
That's where EMDR therapy for addiction becomes especially relevant in a luxury dual-diagnosis setting. It offers a structured way to address the traumatic memories, body reactions, and cue-driven cravings that can keep relapse cycles alive, even in people who are highly motivated and highly accomplished.
High-end residential care matters here. Executives, founders, physicians, attorneys, and public-facing leaders often need discretion, clinical sophistication, and an environment that respects professional obligations. In premium private-pay treatment, privacy isn't an extra. It's foundational. So is comfort. Programs designed for this population may offer private rooms in both detox and residential treatment, along with appropriate access to electronics such as phones and laptops so clients can remain connected to essential work responsibilities while receiving intensive care.
An Advanced Solution for High-Functioning Addiction
At 11 p.m., the presentation is polished, the inbox is under control, and tomorrow's meetings are set. Yet the urge to drink, use, or numb out arrives with a force that feels strangely out of proportion to the day. For many high-functioning adults, that disconnect is the clue. The problem is often less about judgment and more about a nervous system that has learned to treat certain cues as danger.
That pattern matters in executive treatment. A person can be disciplined, insightful, and externally successful, while still being pulled by reactions that begin below conscious thought. Old trauma, unresolved loss, chronic stress, or repeated emotional injury can wire the brain to shift quickly into alarm. Substance use then starts to function like an emergency brake. It brings short-term relief, but it also trains the system to keep reaching for the same answer.
Many professionals miss this link because they use a narrow definition of trauma. In practice, the relevant experiences are often cumulative rather than dramatic. Years of criticism. A chaotic home. Medical fear. Betrayal. Grief that never had room to be processed. Relentless pressure with no real recovery period. The brain does not grade these experiences by résumé status. It registers overload and adapts.
A useful comparison is a smoke alarm set too sensitively. It was installed to protect the building, but now steam from a normal shower can trigger it. In the same way, a tense meeting, a delayed flight, a hotel room, or a sharp email can activate body states that feel urgent and unbearable. The substance is not merely desired. It is recruited.
Clinical reality: High-functioning addiction often reflects an overlearned survival response, not a lack of intelligence or motivation.
EMDR fits this clinical picture because it is a clinically rigorous method for treating trauma-related material that continues to drive present behavior. In a dual-diagnosis setting, it is used to help clients process the memories, sensations, beliefs, and triggers that keep cravings tied to distress. For professionals, that matters because insight alone often cannot reach reactions that are stored in emotional and somatic memory.
It also suits the realities of a demanding life. EMDR does not require a person to give a long, public account of every painful event. In a private, well-run program, treatment can be structured, discreet, and paced carefully around stability, work considerations, and co-occurring psychiatric needs.
The key point is timing. For a high-end client, EMDR works best as one part of an integrated treatment plan, not as an isolated technique used too early. In luxury dual-diagnosis care, the first task is often to build enough internal steadiness that trauma processing can help rather than overwhelm. That is the nuance many general overviews miss, and it is often the difference between temporary symptom relief and durable recovery.
How EMDR Reprograms the Brain's Response to Cravings
Cravings can seem mysterious if they're viewed only as bad habits. They make more sense when they're understood as learned brain responses. A smell, image, conflict, or body sensation can activate a whole chain of memory, emotion, and expectation within seconds. The person doesn't just remember using. The person feels pulled toward it.
The brain as a library
A useful analogy is a library with damaged filing systems. In a healthy system, difficult memories are stored in a way that allows a person to remember them without being overwhelmed by them. In a traumatized system, some files are misplaced, emotionally charged, and too easy to retrieve. When the wrong cue appears, the brain grabs the whole distress package.
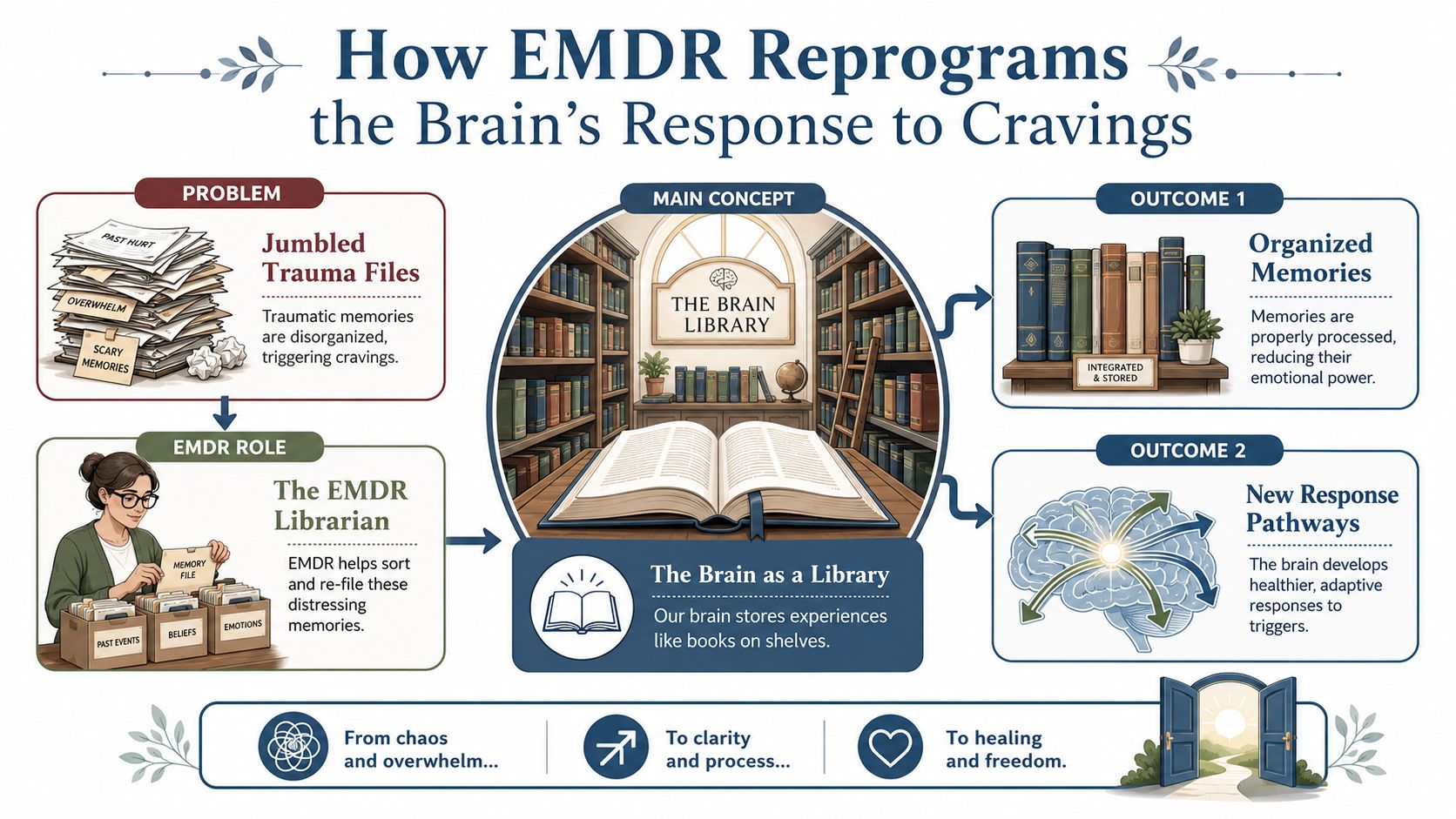
EMDR helps the brain reprocess those files. During treatment, the client briefly holds a target memory, belief, image, urge, or body sensation in mind while following structured bilateral stimulation, often eye movements. The memory isn't erased. It's reconsolidated in a less reactive form.
A recent meta-analysis found that EMDR has moderate-to-high clinical efficacy in reducing addiction-related cravings, with a Hedges' g of 0.55, and that it also significantly reduces comorbid PTSD, depression, and anxiety symptoms in substance use disorder populations, as described in this Frontiers meta-analysis on EMDR for craving and comorbid symptoms.
What reconsolidation means in plain language
Reconsolidation sounds technical, but the basic idea is straightforward. The brain retrieves an old pattern, works with it under new conditions, and stores it again differently. In addiction treatment, that matters because many cravings are attached to old mental representations that still signal relief, escape, or survival.
After effective EMDR work, a client may still remember the event, the person, the place, or the old using ritual. But the cue no longer lands with the same urgency.
A simplified progression often looks like this:
- A trigger activates distress. An argument, shame spiral, or memory appears.
- The old network lights up. The brain predicts that a substance will regulate the state.
- EMDR reprocesses the target. Bilateral stimulation helps the client metabolize the memory.
- The meaning changes. The cue loses some of its emotional force.
- Craving weakens. There's more psychological space between trigger and action.
A useful way to think about EMDR is that it helps the brain stop treating the past as if it's still happening now.
Why this matters in executive recovery
Professionals often respond well when treatment is both experiential and rational. EMDR gives them a framework that's structured enough to trust and efficient enough to respect time. It can address the emotional, cognitive, and body-based layers of craving without reducing recovery to simple willpower.
That difference is often what allows a person to stop white-knuckling sobriety and start experiencing genuine internal change.
The Structured 8-Phase EMDR Process for Addiction
EMDR works best when it follows a disciplined method. That structure reassures many professionals because it's not improvisational and it's not emotionally reckless. It proceeds in phases, with each phase serving a distinct clinical purpose.
EMDR follows an eight-phase approach that allows patients to reframe traumatic memories without requiring detailed verbal retelling, which is one reason it's well suited to professionals who want focused, non-intrusive care, as outlined in this overview of the eight phases of EMDR. For a broader explanation of how trauma-focused work functions in practice, this guide to EMDR therapy for trauma is also a useful companion.
The eight phases in real clinical terms
| Phase | What happens | Why it matters in addiction care |
|---|---|---|
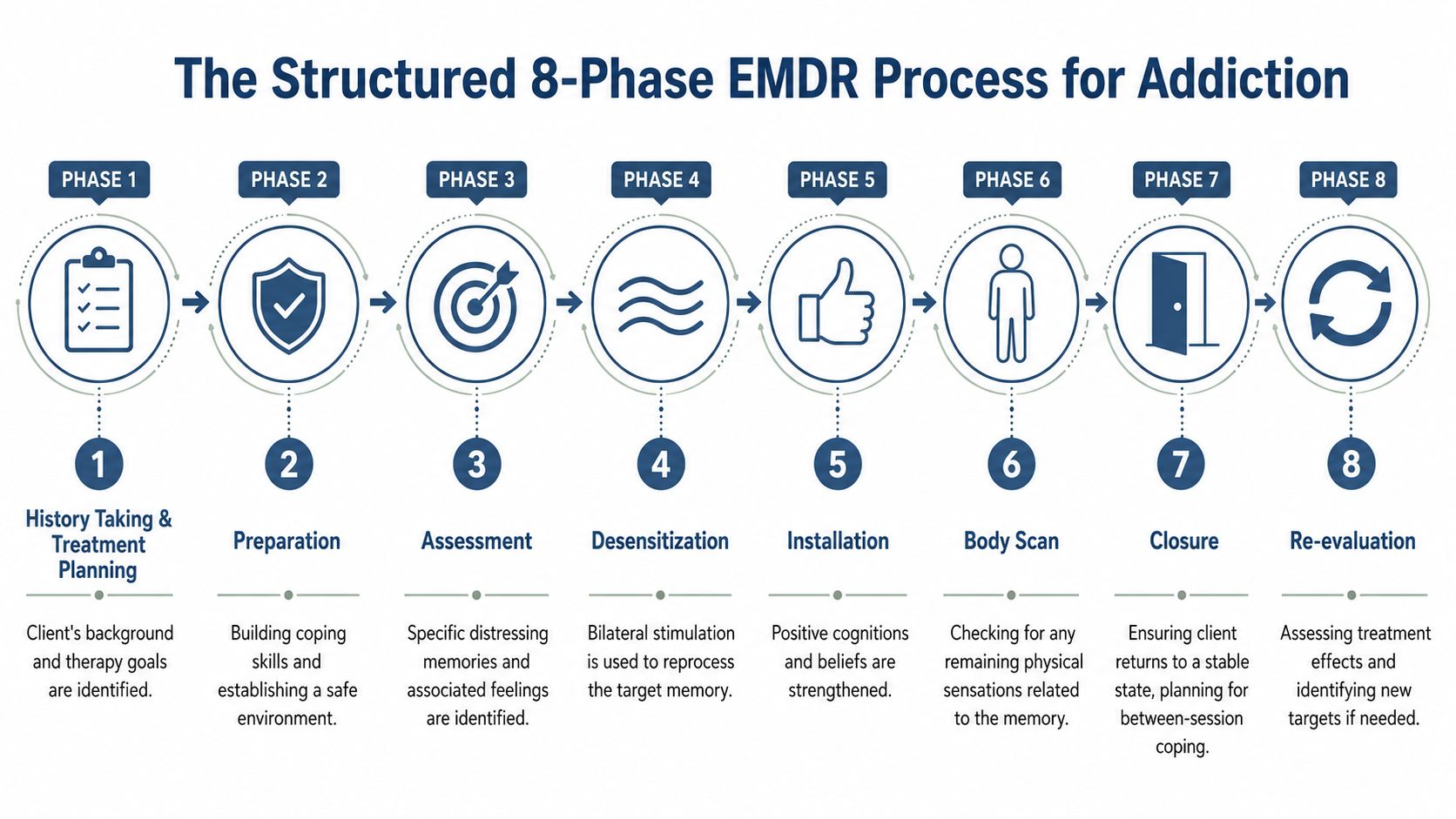
| 1. History taking | The clinician maps trauma history, addiction patterns, triggers, risks, and treatment goals. | It prevents shallow treatment planning. |
| 2. Preparation | The client learns grounding, containment, emotional regulation, and session safety skills. | It builds stability before deeper work begins. |
| 3. Assessment | A specific target is selected, including image, belief, emotion, and body sensation. | It keeps treatment precise rather than vague. |
| 4. Desensitization | Bilateral stimulation is used while the target is processed. | This is where reprocessing begins. |
| 5. Installation | Adaptive beliefs are strengthened. | The client moves from shame or helplessness toward healthier self-perception. |
| 6. Body scan | Residual body activation is checked. | Addiction often lives in the body, not just in thoughts. |
| 7. Closure | The session ends with stabilization and a plan for between-session coping. | This protects functioning outside the therapy room. |
| 8. Reevaluation | The clinician reviews effects and determines next targets. | Treatment stays responsive and measurable. |
What executives usually appreciate about the process
Not every therapy approach fits a person who needs emotional privacy, efficiency, and a strong clinical frame. EMDR often does because it doesn't require hours of detailed retelling. The client remains engaged, but the process is contained.
Several aspects are especially relevant in luxury treatment settings:
- Discretion: The client can process painful material without narrating every detail.
- Structure: Sessions follow a defined sequence rather than drifting.
- Containment: The therapist tracks readiness and regulation continuously.
- Efficiency: The work can be integrated into a broader treatment week without overwhelming the person.
A common misconception: EMDR is not simply moving the eyes and hoping for relief. The outcome depends on case formulation, timing, and the skill of the clinician guiding the process.
For addiction treatment, this structure also helps separate different targets. One client may need to process a humiliating childhood memory that drives shame-based drinking. Another may need to target a relapse chain involving panic, conflict, and self-criticism. The method is standardized, but the application is individualized.
Why Stabilization Is Critical Before Trauma Processing
A well-designed addiction program doesn't rush clients into trauma reprocessing just because trauma is present. That can backfire. A person in acute withdrawal, extreme emotional volatility, or severe functional instability may not have enough internal control to tolerate deeper trauma work safely.

Research notes that attempting EMDR trauma processing during acute withdrawal or high instability can destabilize patients, and that up to 20 to 30% of EMDR sessions for dual diagnosis may be dedicated to extending Phase 2 stabilization, as discussed in this clinical review of stabilization needs in EMDR for dual diagnosis.
What stabilization actually includes
Stabilization is often misunderstood as delay. In reality, it's treatment. It prepares the nervous system for successful processing. In a trauma-informed addiction setting, that may include:
- Withdrawal management: The body needs to be medically and psychologically steadier before deeper memory work.
- Grounding skills: Clients learn how to return to the present when activated.
- Urge management: The team helps reduce the risk that session material will trigger impulsive use.
- Sleep and regulation support: Exhaustion and dysregulation make processing harder.
- Therapeutic alliance: Trust has to be established before vulnerable material can be handled safely.
A reader looking for a broader framework may benefit from this discussion of trauma-informed therapy principles, which align closely with this phase of care.
Why rushed trauma work can undermine results
High-achieving people often want the most direct route. That mindset helps in business and can hurt in recovery. If a client pushes into Phases 3 through 6 before the body can stay regulated, the session may intensify distress without integrating it. The person then leaves feeling raw, flooded, or more vulnerable to relapse.
Good trauma treatment doesn't move as fast as anxiety wants. It moves as safely as the nervous system allows.
In luxury dual-diagnosis care, stabilization is especially important because many clients arrive after long periods of functioning under intense pressure. They may look composed while carrying severe sleep deprivation, concealed panic, dissociation, or exhaustion. The clinical team's job is to read beyond appearances and pace the work correctly.
Integrating EMDR in an Executive Treatment Program
A senior leader can look composed in a board meeting, answer messages within minutes, and still be running on a nervous system that is stuck in threat mode. In treatment, that distinction matters. The clinical question is not whether someone functions. It is whether that functioning is being held together by overcontrol, substances, avoidance, or relentless stress.
Why EMDR works best inside an integrated clinical program
Addiction with co-occurring trauma usually has more than one driver. A client may drink to blunt hyperarousal, use stimulants to outrun exhaustion, or return to a substance after a work conflict activates old shame or fear. EMDR addresses one part of that chain by helping the brain process the memories, body cues, and trigger networks that keep the cycle active. It does not replace the rest of treatment. It fits into a larger plan built around how addiction operates in real life.
That is especially true in dual-diagnosis care. Trauma processing can reduce the intensity of certain triggers, but clients also need practical relapse prevention, psychiatric assessment, sleep support, and therapies that improve emotional control under pressure. A strong program uses each treatment for its specific job instead of expecting one method to carry the full weight.
A useful way to understand the division of labor is to picture a coordinated medical team. One specialist treats the source of pain. Another helps restore strength and daily function. In the same way, EMDR can target the stored traumatic material linked to cravings, while other therapies help the client recognize patterns, communicate more clearly, and respond differently when stress rises.
For example:
- EMDR helps desensitize trauma-linked triggers and the beliefs attached to them.
- Cognitive and behavioral therapy helps clients test distorted thinking and build realistic relapse prevention plans.
- Skills-based emotion regulation work helps with distress tolerance, impulse control, and conflict management.
- Individual psychotherapy helps examine shame, identity strain, grief, secrecy, and the pressure of carrying authority.
- Somatic and mindfulness-based interventions help clients detect activation in the body before it becomes action.
- Family or couples work helps repair relational patterns that can fuel stress, isolation, and relapse risk.
What executive integration looks like in practice
Executives often need treatment that is clinically deep and operationally realistic. That means privacy is protected, distractions are limited, and the structure still allows for carefully managed contact with work when necessary. The goal is not to recreate business as usual. The goal is to protect treatment while accommodating responsibilities that cannot be abandoned without consequence.
In a well-designed executive setting, EMDR sessions are timed and paced within that larger structure. A client might do trauma-focused work on days when the schedule allows enough space for regulation before and after session. Team members then reinforce the work through check-ins, skills practice, medication management if indicated, and attention to sleep, exercise, and nutrition. That coordination matters because EMDR is most effective when the rest of the day supports integration instead of pulling the person straight back into overload.
This level of care is described in more detail in a luxury rehab program for executives, where treatment planning accounts for privacy, professional obligations, and the realities of high-responsibility roles.
A high-acuity executive program often includes features like these:
| Clinical need | Executive treatment response |
|---|---|
| Privacy concerns | Private accommodations and discreet care processes |
| Co-occurring conditions | Integrated psychiatric, addiction, and trauma treatment |
| High cognitive complexity | Nuanced, evidence-based therapies with clear rationale |
| Limited ability to disconnect fully | Structured access to devices for necessary communication |
| Persistent overactivation | Quiet surroundings and schedules that lower baseline stress |
The deeper point is simple. Effective executive treatment does not confuse capability with stability. It respects intelligence, protects confidentiality, and builds a plan that addresses trauma and addiction together without ignoring the demands of a high-stakes professional life.
Recovery for professionals works best when treatment respects competence, while directly treating the patterns that competence alone could not solve.
Measurable Outcomes and What to Expect During Treatment
Results-oriented clients usually ask two questions early. Does this work, and how long does it take? EMDR is appealing partly because it can produce meaningful change without becoming an endless process.
The average treatment duration for EMDR in addiction recovery is 6 to 12 sessions, allowing many professionals to complete intensive trauma-focused work within 6 to 12 weeks, as described in this overview of EMDR treatment duration in addiction recovery.
What clients often notice during the process
EMDR doesn't feel the same for everyone, but some themes are common. A client may begin a session with a specific memory, urge, body tension, or negative belief. As processing continues, the memory often shifts. New associations emerge. The emotional charge may drop. The body may feel less braced.
The experience is often less dramatic than people expect. It's usually not a theatrical breakthrough. It's more often a gradual change in how the brain and body respond.
Clients frequently describe changes such as:
- Less urgency around triggers: The cue appears, but it doesn't command behavior in the same way.
- Improved emotional range: Shame, panic, or anger become more manageable.
- Greater clarity: Patterns that once felt automatic start to become understandable.
- Increased choice: There's more space between distress and the impulse to use.
What outcomes mean in a luxury residential setting
In a premium executive program, these shifts are easier to consolidate because the environment supports them. A client isn't trying to do trauma work alone between board meetings, public appearances, or family crises. The person has clinical containment, privacy, and consistent support.
A realistic expectation is progress, not instant perfection. Some targets resolve quickly. Others require slower work, especially when trauma is layered and longstanding. What matters is that treatment is measurable in daily function: fewer cue-driven reactions, stronger self-regulation, better sleep, more honest communication, and greater ability to sustain recovery under pressure.
Practical rule: The best marker of progress isn't whether a client feels emotional in session. It's whether life becomes less governed by triggers afterward.
Finding a Qualified EMDR Provider for Addiction Recovery
The quality of the provider matters as much as the modality. EMDR can be highly effective for addiction when it's delivered by a clinician who understands trauma, substance use, pacing, and dual-diagnosis complexity. A general therapist with limited addiction training may miss important safety issues.
What to look for
A strong provider or program should show clear competence in both trauma treatment and addiction care. Useful questions include:
- Training and certification: Does the clinician have formal EMDR training and recognized certification?
- Dual-diagnosis experience: Has the clinician treated clients with both trauma symptoms and substance use disorders?
- Stabilization approach: How does the provider decide when a client is ready for deeper trauma processing?
- Residential coordination: If the client is in treatment, how does the EMDR therapist coordinate with medical, psychiatric, and addiction staff?
- Relapse planning: How are post-session vulnerability and craving risk managed?
Why integrated care is often safer for complex cases
For straightforward outpatient concerns, individual EMDR may be sufficient. For executives with active addiction, concealed trauma, sleep disruption, mood symptoms, or relapse risk, a multidisciplinary residential setting is often stronger. It creates one coordinated plan rather than several disconnected ones.
That matters because trauma processing can affect mood, sleep, urges, and interpersonal functioning. When the therapist, psychiatrist, addiction counselor, and residential staff are aligned, they can respond in real time. The client doesn't have to carry the burden of coordinating care while trying to heal.
For readers evaluating premium trauma-focused residential options, this overview of luxury trauma-informed care with EMDR and somatic experiencing for VIPs highlights the level of specialization worth seeking.
The right provider won't promise instant transformation. The right provider will offer disciplined assessment, thoughtful timing, strong containment, and a treatment environment capable of matching the complexity of the case.
Reflections provides confidential, California-licensed luxury dual-diagnosis treatment for professionals, executives, and other high-profile adults who need clinically rigorous care without sacrificing privacy or dignity. In a private residential setting with private rooms in both detox and rehab, a highly accredited multidisciplinary team delivers advanced trauma and addiction treatment while allowing appropriate access to electronics so residents can stay connected to essential career obligations. Those seeking best-in-class private-pay care can learn more about Reflections.









