A senior executive can look successful from the outside and still know something is off. Meetings take more effort than they used to. Decisions that once felt crisp now feel sticky. A short email from a colleague lands like a threat, not a routine update. Sleep becomes lighter. Patience gets thinner. Alcohol, sedatives, stimulants, or rigid routines start doing more emotional work than anyone around them realizes.
Many high performers call this burnout because burnout feels respectable. Sometimes that label fits. Sometimes it doesn't. When stress reactions are rooted in unresolved trauma, the problem isn't a lack of discipline or resilience. It's a nervous system that has learned to stay on guard, even in boardrooms, family conversations, and moments that should feel neutral. For professionals balancing pressure, privacy, and reputation, what is trauma informed therapy becomes a practical question, not an abstract one.
Beyond Burnout Understanding Trauma's Impact on Your Career

A high-functioning professional often notices the change before anyone else does. The calendar is still full. Revenue is still moving. The public face remains polished. Yet focus slips during critical conversations, memory feels less reliable under pressure, and ordinary disagreement triggers an outsized internal response.
That pattern doesn't always look like classic trauma in the popular sense. It may show up as relentless vigilance, difficulty delegating, abrupt emotional withdrawal, or a private dependence on substances to quiet the system after a high-stakes day. In working professionals, unresolved trauma often hides behind productivity until performance starts to narrow.
For many executives, this overlaps with the dynamic explored in executive burnout and addiction. The distinction matters. Burnout usually follows chronic overload. Trauma can make overload feel existential. The body reacts as if every setback threatens survival, which changes how a person thinks, reacts, leads, and recovers.
When performance declines but capability hasn't disappeared
Trauma can disrupt the functions professionals rely on most:
- Attention control that holds steady in long negotiations
- Working memory needed to track competing variables
- Emotional regulation during conflict or scrutiny
- Relational judgment with teams, boards, clients, and family
- Cognitive flexibility when plans shift unexpectedly
Those aren't soft concerns. They're leadership functions.
High achievers often don't need motivation. They need their nervous system to stop treating ordinary professional stress like a live threat.
Why trauma-informed therapy fits this population
Trauma-informed therapy doesn't begin with pathology or labels. It begins with context. It asks whether the mind and body are reacting intelligently to experiences that were never fully processed, rather than assuming a character flaw, a willpower problem, or simple overwork.
That makes it especially relevant for executives, founders, physicians, attorneys, and other professionals who are used to being competent everywhere else. An advanced treatment approach doesn't strip away that competence. It helps restore access to it.
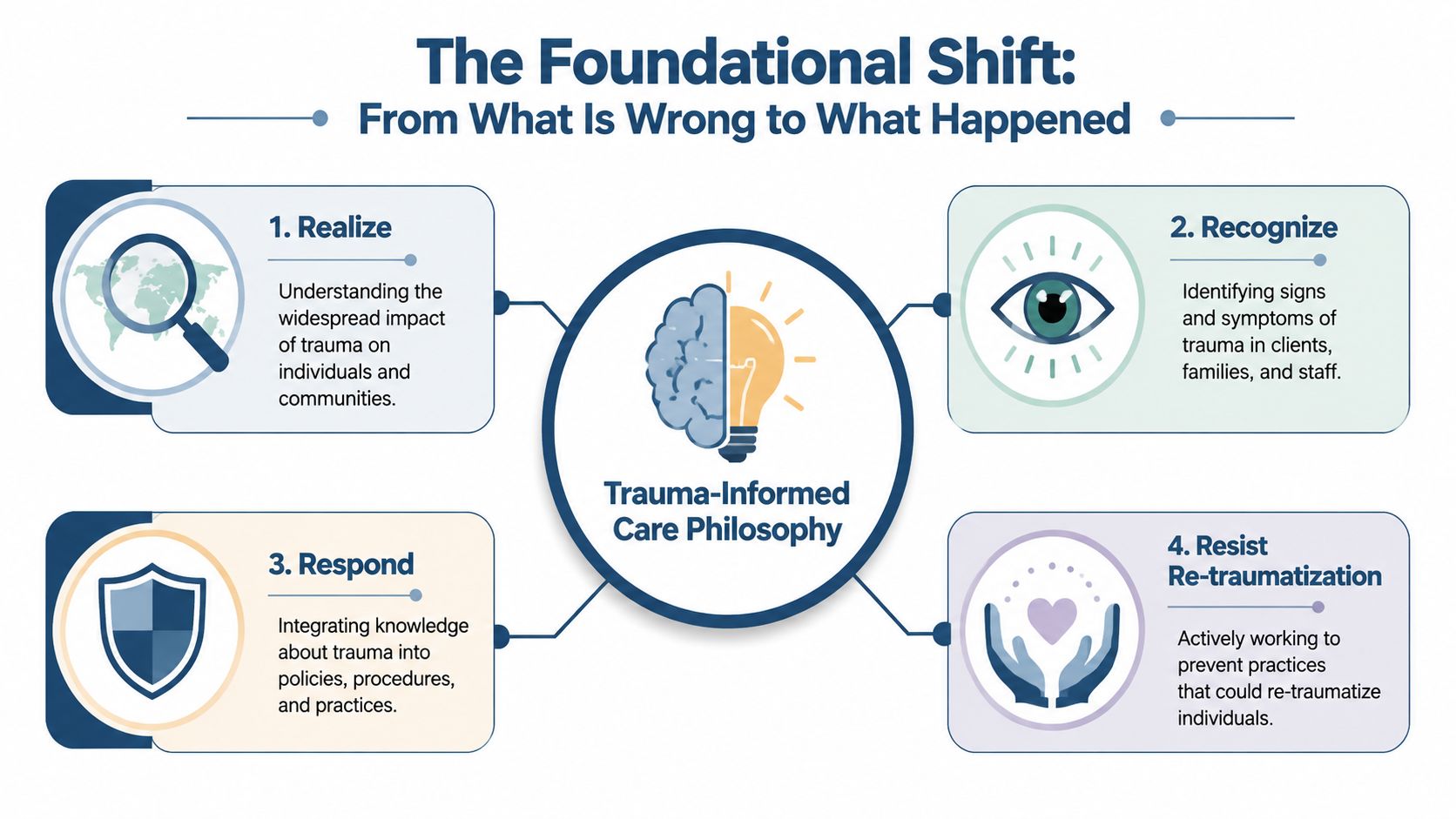
The Foundational Shift From What Is Wrong to What Happened
The defining shift in trauma-informed care is simple and profound. The trauma-informed framework requires clinicians to shift the diagnostic inquiry from "What is wrong with you?" to "What happened to you?". It is operationally defined by four key actions: Realizing the impact of trauma, Recognizing its signs, Responding by integrating this knowledge into practice, and actively Resisting Re-traumatization.
In practice, that changes everything about the clinical atmosphere. The therapist doesn't rush disclosure. Staff don't use confrontation as a shortcut. Treatment planning doesn't reduce a person to a diagnosis. A luxury setting should make that philosophy visible in concrete ways, especially for clients whose lives require discretion, continuity, and adult respect.
The four Rs in real clinical terms
Realize means the team understands trauma is common and often hidden. A polished résumé, public stature, or intellectual sophistication doesn't protect someone from trauma's effects.
Recognize means clinicians know what trauma can look like when it doesn't announce itself. Irritability, over-control, avoidance, substance use, perfectionism, or emotional detachment may all be adaptations rather than simple resistance.
Respond means trauma knowledge changes actual care. Intake, therapy pace, medication discussions, group expectations, and communication style all reflect that understanding.
Resist re-traumatization means the setting avoids repeating the dynamics that injured the client in the first place. Coercion, shaming, power games, unpredictability, and unnecessary exposure are not treatment.
The six principles that make the framework tangible
A strong trauma-informed program is built on six practical pillars drawn from SAMHSA's framework:
- Safety so the client can settle enough to think clearly
- Trustworthiness and transparency so treatment doesn't feel opaque or manipulative
- Peer support so isolation starts to loosen
- Collaboration and mutuality so the client isn't treated like a passive subject
- Fostering client agency, voice, and choice so autonomy is preserved
- Cultural humility so identity and lived context shape care, not assumptions
A concise outside explanation of the principles of trauma-informed healing can be useful for readers who want a parallel description of these fundamentals in plain language.
Clinical reality: A trauma-informed environment is not indulgent. It's structured in a way that allows difficult treatment to happen without unnecessary destabilization.
For discerning clients, this is often what distinguishes a therapeutic setting from a polished but emotionally tone-deaf one. Expensive surroundings alone don't make care trauma-informed. The deciding factor is whether every layer of treatment protects dignity while supporting meaningful psychological work.
Understanding a Critical Distinction for Your Recovery
Many people use the terms interchangeably, and that creates expensive confusion. Trauma-informed care and trauma-focused therapy are related, but they aren't the same thing.

The clearest comparison is this. Trauma-informed care is the operating room. Trauma-focused therapy is the surgical procedure. A first-rate operating room matters. It must be safe, organized, and prepared. But safety alone doesn't perform the surgery.
Side-by-side difference that clients should understand
| Trauma-informed care | Trauma-focused therapy |
|---|---|
| A clinical framework that shapes the environment, relationships, and pacing of care | A direct intervention designed to process traumatic memories and reduce trauma symptoms |
| Applies broadly, including to people who may not need memory-processing work | Used when a person needs focused treatment for trauma-related symptoms |
| Emphasizes safety, collaboration, autonomy, and prevention of re-traumatization | Uses specialized methods such as EMDR or TF-CBT when clinically appropriate |
That distinction matters because some programs market "trauma-informed" as if it automatically includes trauma processing. It doesn't.
According to the AAP overview of trauma-informed care, 40-50% of adults with PTSD require specific trauma-focused modalities like EMDR or TF-CBT to process traumatic memories and achieve symptom reduction. For a client with significant trauma symptoms, safety is necessary but incomplete.
What this means for a professional evaluating treatment
A high-achieving adult should ask two separate questions.
First, is the program trauma-informed in how it conducts treatment?
Second, does the program provide trauma-focused modalities when they're clinically indicated?
Those are different standards. A calm setting, respectful staff, and excellent hospitality do not substitute for specialized trauma work. At the same time, trauma-focused methods delivered in a rushed, misattuned environment can backfire.
For readers wanting another perspective specific to women seeking advanced care, this women's trauma care guide in Italy offers a useful example of how trauma-sensitive framing can be adapted to a distinct client population.
The best programs don't force a choice between safety and depth. They provide both.
For executives and other high-visibility clients, that precision protects against a common mistake. They enter treatment expecting root-cause work, only to find a supportive environment with no real mechanism for processing trauma. Clarity on this point saves time, money, and unnecessary disappointment.
Your Journey Through Assessment and Therapy Sessions
In a high-end clinical setting, assessment should feel like a disciplined conversation, not a forensic extraction of private pain. The first task is to establish psychological safety and professional trust. That matters even more for clients whose daily lives involve confidentiality, leadership demands, and little margin for public disruption.
The early phase of treatment should answer quiet but important questions. Will this team respect boundaries? Will they understand the difference between privacy and avoidance? Can difficult work happen without destabilizing professional obligations or treating those obligations as denial?
What the initial assessment should feel like
The best trauma-informed assessments are structured, but not invasive. Clinicians gather history, mental health symptoms, substance use patterns, medical considerations, sleep, stress load, family dynamics, and professional demands. They do that while tracking the client's level of activation, not merely the content of the story.
A key point often surprises people: trauma-informed protocols utilize neurobiological interventions to regulate the amygdala and prefrontal cortex, and they technically do not require disclosure of explicit traumatic details until a patient is ready, which has been shown to reduce re-traumatization incidents in clinical settings by up to 50%. In other words, the client doesn't have to prove the seriousness of the trauma by recounting everything at once.
A sophisticated assessment looks for readiness, regulation, and pattern recognition before it pushes for detail.
Many high-functioning adults then begin to exhale. They realize treatment can be both serious and measured.
What happens inside sessions
Sessions often begin with stabilization rather than immediate memory work. That can include psychoeducation on stress responses, grounding exercises, and methods that help the client distinguish present reality from old threat cues. These are not superficial coping tricks. They help restore enough internal order for deeper work to proceed intelligently.
Depending on clinical need, treatment may include:
- Nervous system regulation through grounding, breath pacing, sensory orientation, and body-based awareness
- Cognitive work to address trauma-linked beliefs such as guilt, shame, danger, or mistrust
- Relational work that helps the client practice collaboration instead of defensive control
- Trauma processing when indicated and timed appropriately
For clients considering modalities that involve body-based processing, a focused explanation of somatic experiencing in treatment can help clarify how nonverbal trauma responses are addressed.
Another useful overview for readers weighing memory-processing options is this Providers for Healthy Living EMDR guide, particularly because many professionals want to know whether trauma treatment always requires exhaustive verbal retelling. It doesn't.
Why luxury logistics matter in real recovery
For executives, physicians, entrepreneurs, and high-level operators, treatment can't be designed as if real life stops. In premium private-pay settings, practical details often determine whether a client can fully engage.
A clinically mature program may include features such as:
- Private rooms in detox and residential care so clients can decompress without constant social exposure
- Appropriate access to electronics including phones and laptops, allowing continued contact with essential work responsibilities
- Discreet scheduling and communication protocols to protect reputation and confidentiality
- A multidisciplinary team capable of handling dual-diagnosis complexity without fragmenting care
Those features aren't luxuries in the trivial sense. For this population, they're part of making treatment viable. A client who can maintain key responsibilities in a bounded, clinically supervised way is often less defended and more willing to do serious work. The structure has to fit the life, or the life will overwhelm the structure.
Evidence Based Outcomes for Lasting Resilience
Executives rarely ask only whether treatment feels supportive. They want to know whether it works. That is a reasonable standard.
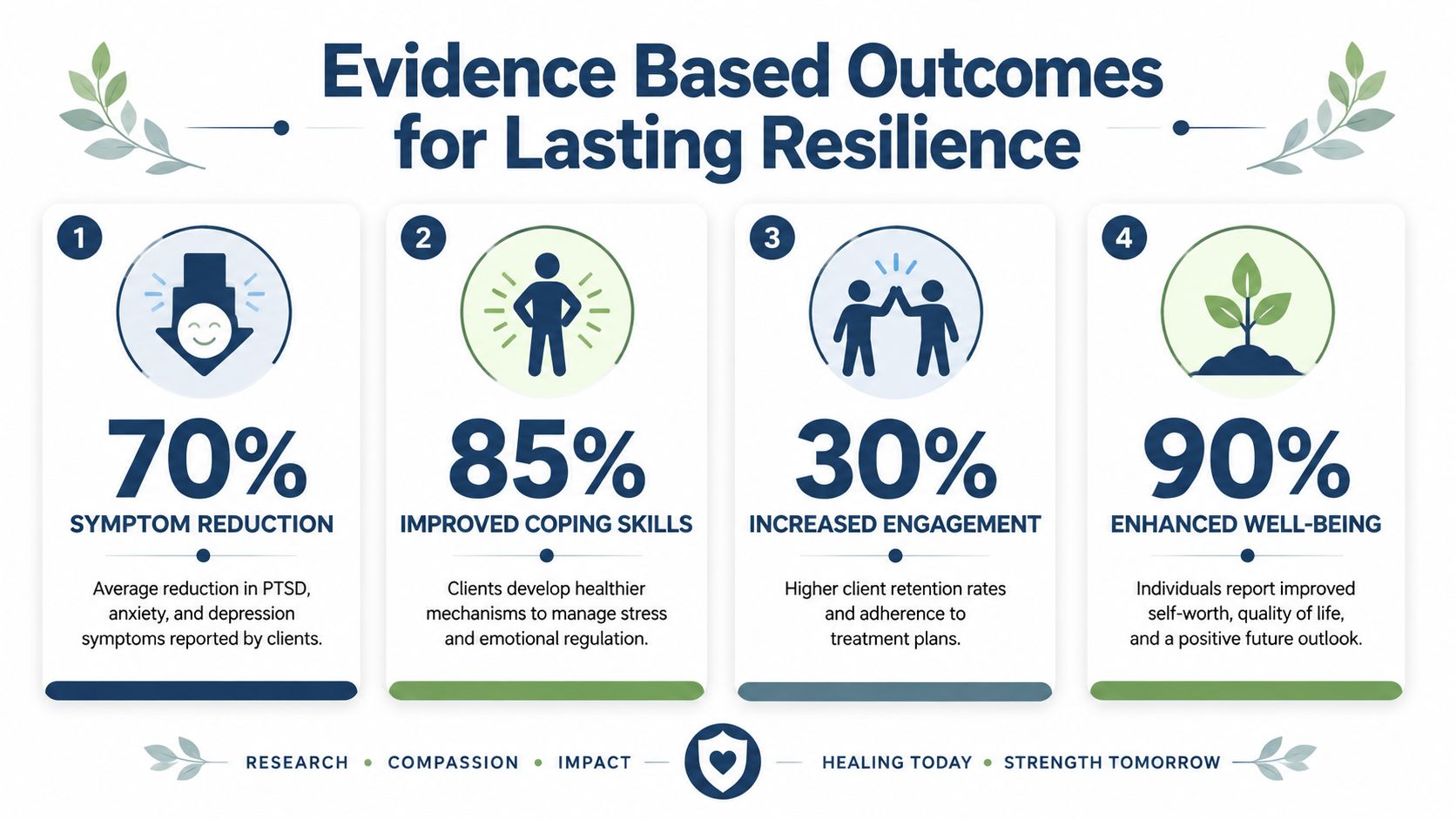
The strongest quantitative finding available here is substantial. A 2023 meta-analysis in Psychological Medicine found that patients in trauma-informed therapy experienced a 40% greater reduction in PTSD symptom severity compared to standard care groups, with outcomes showing sustained recovery for up to one year post-treatment. That finding appears in the verified data provided for this article and is central to understanding why this framework has become so important.
Translating symptom change into professional function
Clinical outcomes matter because they shape daily performance. When trauma symptoms recede, professionals often regain capacities that seemed mysteriously unavailable under pressure.
Those gains may include:
- Cleaner decision-making because threat reactivity isn't constantly crowding out judgment
- Better concentration during complex tasks and negotiations
- More stable emotional range in conflict, leadership, and family life
- Improved trust calibration so relationships are neither overly guarded nor naively open
- Reduced dependence on substances or compulsive coping used to manage internal overload
A symptom score is not the whole story. What matters to a discerning client is whether cognitive bandwidth returns. Can the person tolerate uncertainty again? Can they sit in a hard meeting without going numb, exploding, or reaching for chemical relief later? Can they lead without burning through themselves?
What lasting resilience actually looks like
Resilience is often described too vaguely. In advanced treatment, it isn't stoicism. It is the restored ability to stay present, think clearly, and choose deliberately when stress rises.
Recovery is durable when the client gains both insight and regulation. Insight without regulation leaves a person informed but still overwhelmed.
For high-performing adults, the practical markers of progress are often subtle at first. Fewer overreactions. Less decision paralysis. Greater tolerance for feedback. Better sleep. More flexible thinking. A noticeable drop in the private effort required to appear composed.
The broader context also matters. The verified evidence notes that trauma is common, and that trauma-informed treatment was associated with significant reductions in PTSD, depression, and anxiety in the reviewed literature. That helps explain why a trauma-sensitive framework has become clinically relevant far beyond narrowly defined PTSD care.
The business case and the human case are the same. When unresolved trauma drives executive dysfunction, treating it is not a retreat from professional life. It's a restoration of the capacities that make professional life sustainable.
How to Evaluate Providers and Ask the Right Questions
A discerning client shouldn't evaluate treatment the way someone shops for amenities. The right question isn't whether a program looks impressive. It's whether the clinical structure is strong enough, private enough, and flexible enough to treat complex trauma and co-occurring substance use without creating new problems.
Accreditation is a starting point, not a finishing point. A helpful overview of Joint Commission accreditation standards can clarify why external quality review matters. But polished credentials still need to be matched by real trauma competence.
What to verify before making a commitment
Look for a provider that can demonstrate the following:
- Accredited clinical operations with clear standards for safety, documentation, and quality oversight
- A multidisciplinary team that includes doctoral-level or otherwise highly specialized mental health leadership, psychiatry, addiction expertise, and trauma-capable therapists
- Dual-diagnosis fluency so trauma, mood symptoms, anxiety, and substance use are treated together rather than in isolation
- A true trauma-informed environment rather than a marketing label attached to otherwise generic care
- Access to trauma-focused modalities when those methods are clinically indicated
- Private accommodations and strong confidentiality protocols for clients who require discretion
- A realistic policy for professional continuity when work obligations can't be suspended entirely
Intelligent questions to ask an admissions team
Not every important question appears on a website. Ask directly.
How is trauma-informed care reflected in the actual patient experience?
Listen for specifics about assessment pace, staff communication, privacy, collaboration, and prevention of re-traumatization.Which trauma-focused therapies are available when clinically needed?
A serious provider should be able to name the modalities used and explain how timing is determined.How do you handle co-occurring substance use and trauma at the same time?
Sequential treatment often fails clients whose substance use functions as trauma management.What privacy protections are in place for executives, public figures, and licensed professionals?
General assurances aren't enough. The answer should include operational boundaries.Are private rooms available in both detox and residential treatment?
For many professionals, environmental control is not vanity. It supports regulation and sleep.Can residents maintain limited access to phones and laptops for essential responsibilities?
In premium care, the right answer is often nuanced rather than rigid. Clinical boundaries should coexist with real-world obligations.How is family involvement handled when the client wants discretion?
Families can help recovery, but involvement should be purposeful and well managed.
Decision rule: If a program can describe its trauma philosophy but can't explain its trauma methods, the picture is incomplete.
The best luxury programs don't ask accomplished adults to surrender judgment at the door. They expect informed questions. They answer them clearly. They understand that expensive private-pay care should deliver both hospitality and rigor.
For professionals who need discreet, clinically advanced treatment without stepping away from every responsibility, Reflections offers Joint Commission accredited luxury dual-diagnosis care in a private residential setting. Clients receive private rooms in both detox and rehab, treatment from a highly credentialed multidisciplinary team, and appropriate access to electronics so essential work and family obligations can continue while meaningful recovery begins.









