A senior leader closes the laptop after another late call, pours a drink, and tells himself it's just to take the edge off. Sleep has been thin for months. Certain emails trigger a surge of adrenaline that doesn't match the moment. A loud sound in a restaurant feels disproportionate. Irritability shows up in meetings, then disappears behind polished performance. From the outside, everything still looks intact.
That private split is common in high-functioning professionals dealing with PTSD and alcohol addiction. Career success can hide a great deal. Discipline, stamina, and a high tolerance for pressure often delay recognition of what's happening underneath. By the time alcohol becomes the nightly way to quiet intrusive thoughts, blunt hypervigilance, or force sleep, the pattern can feel less like a choice and more like a system that's taken over.
For executives, the barriers to getting help are often different from the barriers faced by the general public. The question usually isn't whether treatment exists. It's whether treatment can be discreet, clinically advanced, and compatible with real-world responsibilities. It can.
The Unseen Struggle for High-Achieving Professionals

The executive version of trauma rarely looks dramatic at first. It often looks efficient. The person still makes decisions, still boards flights, still answers difficult questions under pressure. What changes is the cost of maintaining that performance. Alcohol becomes the transition tool after high-stakes meetings, before bed, during travel, or before events that demand social ease.
When success conceals clinical risk
Many professionals with trauma histories don't identify with the stereotype of addiction. They aren't drinking in public view. They're controlling the optics, keeping commitments, and compensating harder. That's one reason this dual condition can progress subtly until concentration slips, relationships strain, or physical dependence begins to shape the day.
The clinical overlap is substantial. The U.S. VA National Center for PTSD reports that 45% of adults with PTSD also have problems with drug or alcohol use, and research reviews show comorbidity rates ranging from 28% to 75%, which is why integrated treatment matters so much in practice (VA PTSD substance misuse overview).
Practical rule: If alcohol has become the primary way to turn down trauma symptoms, the issue isn't a lack of discipline. It's a co-occurring condition that needs treatment designed for both problems at once.
Why professionals delay treatment
The hesitation usually comes from understandable concerns:
- Confidentiality concerns: Executives worry about reputation, licensing, leadership visibility, and unwanted disclosure.
- Operational pressure: Many feel they can't step away without creating risk for staff, clients, investors, or family obligations.
- Identity conflict: High performers are used to being the stabilizing force. Asking for help can feel incompatible with that role.
A treatment setting built for this population has to account for all three. Programs designed for working professionals in residential treatment are often a better fit because they recognize that privacy and career continuity aren't luxury extras for this group. They're part of whether treatment is realistic at all.
What matters most at this stage is recognizing the pattern without shame. PTSD and alcohol addiction are treatable. The need for discreet care doesn't make the problem less serious. It means the treatment environment has to match the life the person is trying to protect.
Why PTSD and Alcohol Addiction Occur Together
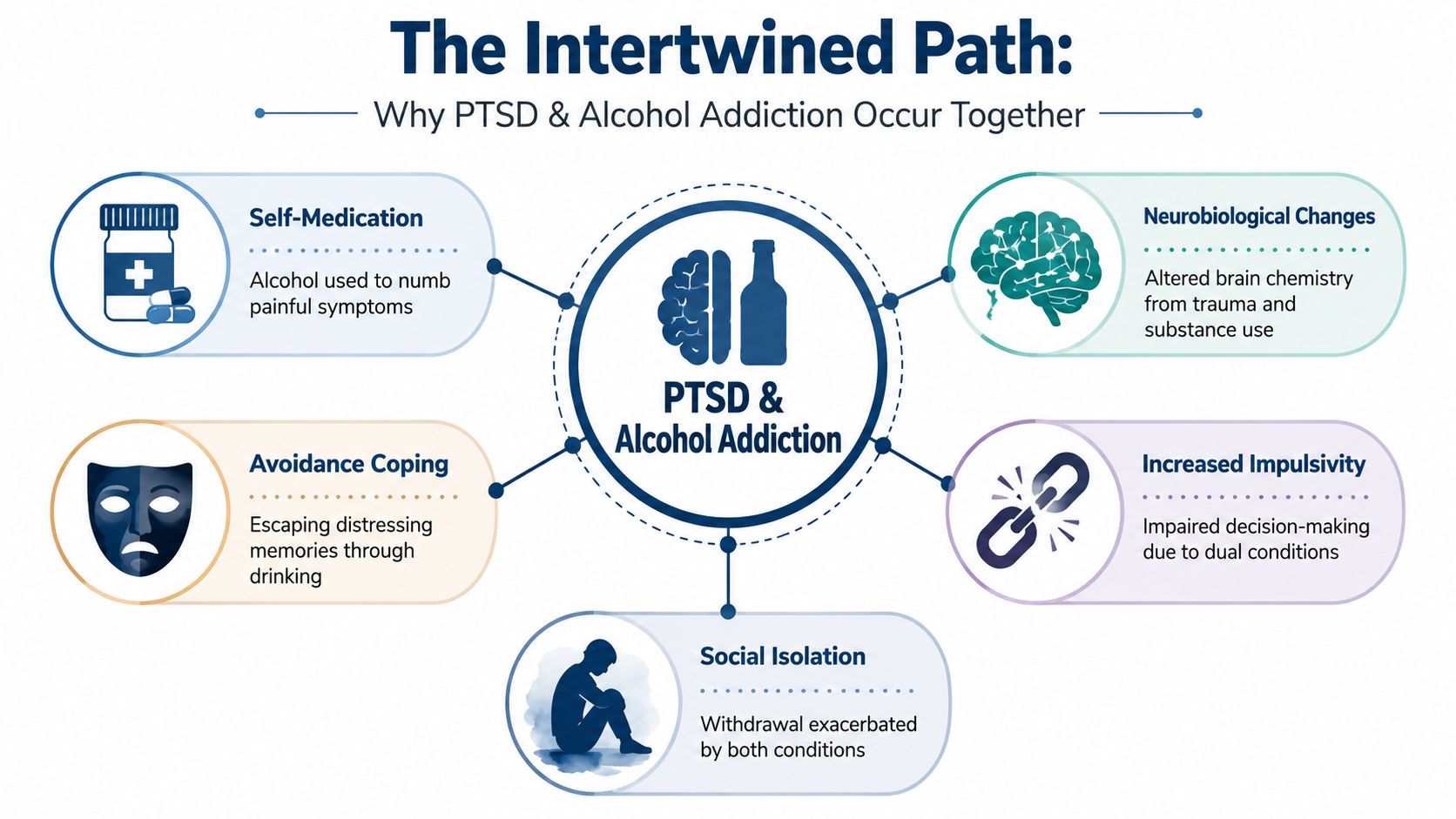
The core mechanism is straightforward. Alcohol works quickly. It can temporarily dull physiological arousal, narrow attention, and create short-term emotional distance from distressing memories or sensations. For someone living with trauma symptoms, that immediate relief can feel highly functional. It isn't.
Alcohol often becomes a coping tool
Researchers have identified coping-motive drinking as a central link between trauma symptoms and harmful alcohol use. A meta-analysis found that coping-motive drinking accounted for 80% of the total effect linking PTSD to harmful alcohol use (meta-analysis on coping motives and PTSD). In plain terms, many people aren't drinking randomly or purely socially. They're drinking to manage internal states they don't know how to regulate any other way.
That pattern usually follows a recognizable sequence:
- A trauma symptom appears. It may be insomnia, agitation, intrusive imagery, emotional numbing, or a sense of being constantly on guard.
- Alcohol provides short relief. The person feels calmer, sleepier, less emotionally flooded, or less mentally preoccupied.
- The brain learns the shortcut. Over time, distress and drinking become linked.
- The original symptoms worsen. Sleep quality declines, emotional volatility increases, and the person has fewer sober opportunities to build durable coping skills.
The cycle isn't only psychological
Trauma affects attention, threat detection, mood regulation, and behavior. Alcohol complicates each one. A professional who already feels overstimulated may become more impulsive, more avoidant, or more isolated once drinking is added to the picture. That makes the workday harder, not easier, even if the nightly drink still feels “necessary.”
A few patterns show up often in clinical practice:
- Avoidance gets reinforced: Drinking helps the person avoid memories, body sensations, or conversations tied to trauma.
- Stress tolerance narrows: The person appears high-functioning, but resilience becomes increasingly dependent on alcohol.
- Isolation grows: More time goes into concealing symptoms, managing hangovers, and limiting situations that might expose the problem.
The trap is that alcohol can feel effective in the short term while steadily reducing a person's ability to recover in the long term.
There's also a more nuanced point that matters for treatment planning. The relationship is bidirectional. Trauma can drive drinking, but alcohol use can also increase vulnerability after traumatic events and complicate how symptoms develop. That's why simplistic education often misses the mark. Not every case fits a one-direction story, and not every successful professional drinks for the same reason.
Recognizing the Signs of a Co-Occurring Disorder
High-achieving adults often miss the pattern because each symptom can be explained away on its own. Poor sleep gets blamed on travel. Irritability gets blamed on pressure. More frequent drinking gets framed as networking, decompressing, or a rough season. A key question is whether these changes are clustering around trauma symptoms.
Signs that show up at work
The earliest indicators are often behavioral rather than dramatic. The person still performs, but the margin of ease disappears.
- More reactivity in meetings: A routine disagreement feels threatening or disproportionately activating.
- Difficulty concentrating on strategic tasks: Attention drifts, especially after poor sleep or after contact with a reminder tied to past trauma.
- Avoidance of certain people or settings: Client dinners, conferences, specific neighborhoods, or travel routes start to feel harder to tolerate.
- Longer recovery after ordinary stress: A tense call triggers hours of internal agitation rather than a brief spike.
Signs that show up in private life
Outside work, the pattern usually becomes clearer. Alcohol starts serving a specific function.
| Pattern | What it can look like |
|---|---|
| Using alcohol to switch states | Drinking to fall asleep, calm down, stop replaying events, or feel normal in social situations |
| Secrecy | Pouring stronger drinks at home, minimizing quantity, or planning the evening around access to alcohol |
| Emotional constriction | Feeling detached with family, less patient with children, or unable to relax without substance use |
| Escalation | Needing more alcohol for the same effect or feeling unsettled on nights without it |
Research also points to a specific craving pathway in this population. Exposure to trauma reminders, not just general stress, produces the largest increase in alcohol craving, directly linking PTSD triggers to drinking behavior (study on trauma cues and alcohol craving).
A useful self-check is timing. If the strongest urge to drink follows a reminder, a nightmare, a conflict that echoes an old wound, or a surge of hypervigilance, that's clinically meaningful.
When to stop calling it stress
A standard “stress problem” usually improves with rest, boundaries, and routine adjustments. A co-occurring disorder tends not to. If alcohol has become the main relief valve and trauma symptoms keep resurfacing despite success, structure, and willpower, that's a sign the issue needs formal assessment.
For professionals, early intervention matters because the consequences often arrive sideways. Not in one public collapse, but in impaired judgment, increasingly brittle relationships, and a growing sense that the person can't fully trust himself under pressure.
Why a Standard Diagnosis Is Not Enough
A basic intake that labels someone with PTSD and alcohol use disorder may be technically correct, but it often isn't clinically sufficient. High-functioning adults need more than a checklist diagnosis. They need a precise map of how the two conditions interact in their specific life.
What a stronger assessment actually answers
A thorough dual-diagnosis evaluation looks beyond symptom presence. It clarifies questions such as:
- What role does alcohol serve right now? Sleep aid, anxiety dampener, emotional anesthesia, social lubricant, or all of the above.
- What activates the trauma response? Certain environments, relational dynamics, sensory reminders, leadership conflict, travel, or isolation.
- What else is in the picture? Depression, panic, grief, chronic stress, or another condition that changes treatment sequencing and risk management.
The relationship between trauma and alcohol isn't one-directional. The link is bidirectional, which is why expert guidance emphasizes screening and treating both conditions concurrently rather than assuming one fully explains the other (PTSD UK overview of PTSD and alcohol).
Why the team matters
A comprehensive evaluation usually requires more than one perspective. Psychiatrists, psychologists, addiction clinicians, and trauma therapists notice different things. One clinician may identify withdrawal risk. Another may spot avoidance patterns that look like perfectionism. Another may recognize that a person's “work stress” is in fact trauma activation in a high-authority environment.
That level of assessment is the foundation of effective dual diagnosis treatment for trauma and addiction. Without it, treatment can become too generic. The person may get advice to stop drinking without learning how to handle flashbacks, nightmares, shame, or physiological overactivation. Or he may begin trauma work without enough support for cravings, sleep disruption, and relapse prevention.
A diagnosis names the problem. A thorough assessment explains how the problem operates in this person's life.
For executives, that distinction matters. They're often making treatment decisions while carrying substantial personal, financial, and professional responsibility. Precision isn't a luxury in that setting. It's what keeps treatment from becoming another interruption that doesn't address the root issue.
How Integrated Treatment Breaks the Cycle
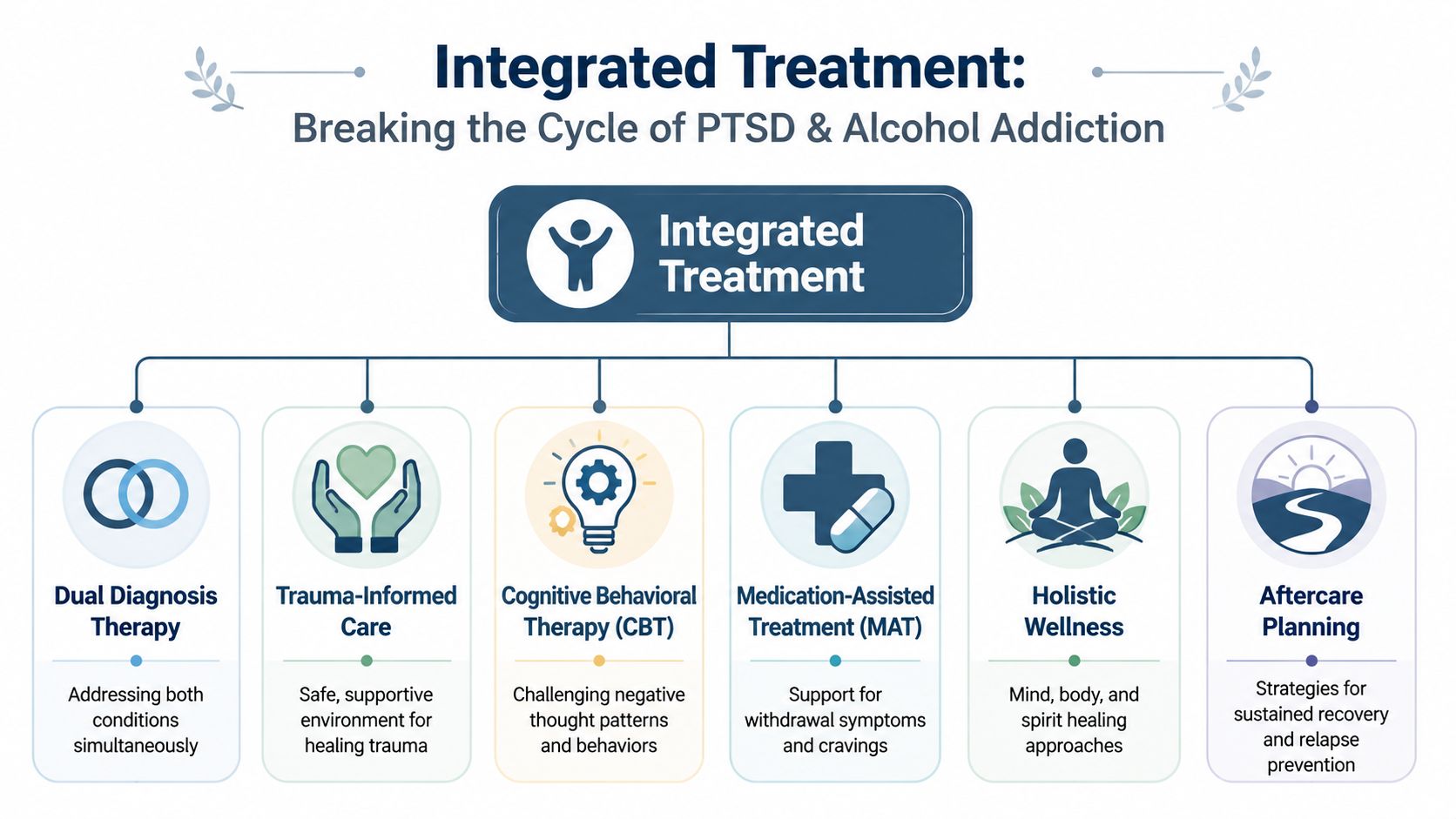
Integrated treatment means both conditions are addressed in the same plan, by the same clinical system, with enough coordination that one problem doesn't sabotage work on the other. That sounds obvious, but many people still arrive after trying partial solutions. They've cut down drinking without touching trauma. Or they've done insight-oriented therapy while cravings and withdrawal were left unmanaged.
What tends not to work
Treating alcohol in isolation often fails when trauma cues continue to drive urge states. Treating PTSD without enough addiction support can also stall when the person keeps using alcohol to regulate distress between sessions.
A more effective model accepts two realities at once:
- Trauma symptoms need direct treatment.
- Alcohol use needs medical, behavioral, and psychological intervention at the same time.
Evidence cited by the VA and ISTSS shows that trauma-focused psychotherapies remain effective for PTSD even when a substance use disorder is present, and integrated treatment can reduce both conditions without making drinking worse (review on integrated treatment for alcohol and PTSD).
What integrated care includes
A strong program usually combines several layers of care rather than relying on one method.
| Component | Why it matters |
|---|---|
| Trauma-focused psychotherapy | Helps process trauma safely and reduce avoidance, intrusive symptoms, and hyperarousal |
| Detox and medication management | Addresses withdrawal risk, sleep disruption, and cravings when clinically appropriate |
| Skills-based therapy | Builds alternatives to drinking through CBT, DBT, emotion regulation, and relapse prevention |
| Holistic interventions | Supports nervous system regulation through mindfulness, movement, somatic work, nutrition, and restorative routines |
| Family work | Repairs trust, improves communication, and reduces the secrecy that often sustains both conditions |
| Aftercare planning | Prepares for travel, leadership stress, social alcohol exposure, and relapse triggers after discharge |
For readers who want a clearer sense of how one core modality works, it can help to explore Vancouver cognitive behavioral therapy options as a general reference on CBT principles and structure.
What this looks like in a professional setting
In a quality dual-diagnosis environment, treatment doesn't rely on generic advice such as “just stop drinking” or “talk about the trauma when you're ready.” It's more operational than that. Clinicians identify cue patterns, restructure routines, reduce physiological overload, and build practical responses for the moments when symptoms usually lead to alcohol.
That often includes:
- Morning stabilization: sleep support, medication review if indicated, and structured planning for the day
- Targeted therapy sessions: work on trauma, shame, coping, and belief systems that keep both conditions active
- Real-life rehearsal: planning for dinners, flights, presentations, difficult calls, and weekends at home
- Continuity of care: a residential or structured setting followed by step-down support and long-term monitoring
Some programs, such as integrated mental health and addiction treatment, are built specifically around this coordinated model. The advantage isn't just convenience. It's clinical coherence. The person doesn't have to split his story into separate boxes or receive conflicting advice from different providers.
Choosing a Treatment Path That Respects Your Career
For executives and other high-visibility professionals, the decision to enter treatment is rarely only about symptoms. It's also about whether care can be received without unnecessary disruption, exposure, or loss of control over critical obligations.
Privacy isn't a preference
This population often needs a setting where treatment feels contained, discreet, and professionally managed. Shared rooms, chaotic environments, and blanket restrictions can become barriers before therapy even begins. Private accommodations matter because they support sleep, emotional decompression, and confidentiality. They also reduce the performative pressure many leaders feel in communal settings.
Another practical issue is technology. Some professionals can't disappear completely. Board responsibilities, legal matters, ownership duties, and family systems may require limited but meaningful communication. In the right setting, access to phones and laptops can be clinically managed rather than automatically prohibited.
What to look for in an executive-appropriate program
A suitable program should balance therapeutic containment with real-world functionality.
- Private rooms in detox and residential care: This supports rest, discretion, and a calmer transition into treatment.
- A multidisciplinary clinical team: Trauma and alcohol addiction require expertise across psychiatry, psychology, and addiction medicine.
- Permission for appropriate electronics use: Professionals may need to maintain select responsibilities while still engaging fully in care.
- A setting that understands reputation risk: Admissions, programming, and discharge planning should reflect the realities of high-profile lives.
A provider such as Reflections offers California-licensed, Joint Commission-accredited residential dual-diagnosis care with private rooms, clinically managed detox, and appropriate access to electronics for adults who need treatment that can coexist with legitimate work obligations. For the executive audience, that structure can make the difference between postponing care and beginning it.
Recovery doesn't require sacrificing a career. It requires choosing a setting that treats privacy, discretion, and clinical depth as part of the treatment itself.
The strategic decision
Professionals are accustomed to solving hard problems by staying in motion. PTSD and alcohol addiction usually don't respond to that approach for long. The more advanced the life, the more expensive delay tends to become. Health deteriorates subtly. Decision-making narrows. Family life absorbs the spillover. Work may still look stable, but the internal system gets less reliable.
The right treatment path protects more than sobriety. It protects judgment, energy, leadership capacity, and the ability to be present at home without relying on alcohol to manage the nervous system. For many successful adults, entering treatment is less a retreat from responsibility than a disciplined correction before the private problem becomes a public one.
A confidential conversation with Reflections can help clarify whether PTSD, alcohol use, or both are driving the current pattern, and what level of discreet, executive-focused care fits best. For professionals who need privacy, private rooms, dual-diagnosis expertise, and the ability to stay appropriately connected to work, that first step can be practical, contained, and fully confidential.









