A successful executive can hide a great deal for a long time. Missed sleep gets explained away as drive. Irritability gets mistaken for intensity. Grand plans sound like vision until they start colliding with reality. Then the cracks widen. A board meeting goes sideways. A spouse sees the mood shift coming before anyone else does. A high performer who's built a life on control starts losing it in private.
That's usually the moment bipolar disorder residential treatment stops sounding extreme and starts sounding necessary.
For professionals, the hardest part isn't only the illness. It's the belief that getting help will destroy momentum, expose vulnerability, or interrupt a career that took decades to build. That belief keeps many people in outpatient care that isn't enough, or in cycles of brief stabilization followed by another unraveling. A premium residential program built for executives solves a different problem than a generic facility. It protects privacy, delivers serious clinical treatment, and makes room for professional continuity instead of forcing a false choice between health and responsibility.
Navigating Bipolar Disorder While Leading a Career
A managing partner notices that a top rainmaker has become impossible to read. One week, that executive is brilliant, fast, and magnetic. The next, the same person is agitated, sleeping poorly, impulsive with money, and combative with people who usually trust their judgment. At home, the family is frightened. At work, the team is confused. The executive keeps saying the pressure will ease after the next launch, next quarter, next deal.
It won't.
Bipolar disorder doesn't respect title, compensation, or reputation. It can sharpen ambition in one phase and sabotage judgment in the next. The damage often shows up first in places high achievers care about most: leadership credibility, family trust, and decision quality.
Why stepping away can be the most responsible move
Residential treatment is often framed as retreat. That's the wrong frame for a successful professional. For the right candidate, it's a strategic intervention. It removes chaos, imposes structure, and gives an accredited clinical team the time and access needed to assess mood patterns, medication response, sleep disruption, substance use, and stress triggers that outpatient care can miss.
Practical rule: If symptoms are affecting judgment, sleep, impulse control, or substance use, waiting for a less busy season is usually a costly mistake.
The professionals who do best in treatment typically stop treating symptoms like a branding problem. They start treating bipolar disorder like any other high-stakes threat. They gather the right experts, commit to a defined plan, and act before the next episode makes the decision for them.
What families and colleagues often see first
The person in the center of the illness may not fully recognize how far things have drifted. Others usually do.
- Family members notice instability at home: sleep changes, conflict, emotional distance, or risky behavior.
- Coworkers see performance distortion: erratic communication, overpromising, sudden reversals, or impulsive strategy shifts.
- The individual feels the internal cost: racing thoughts, exhaustion, shame, or the sense that everything is becoming harder to hold together.
A high-end private-pay program is the right move when discretion matters, when comfort affects willingness to engage, and when treatment must be advanced enough to match the complexity of a professional life. The goal isn't just to get someone through a crisis. The goal is to restore steadiness without dismantling identity, status, and future plans.
What Is Executive Bipolar Disorder Residential Treatment
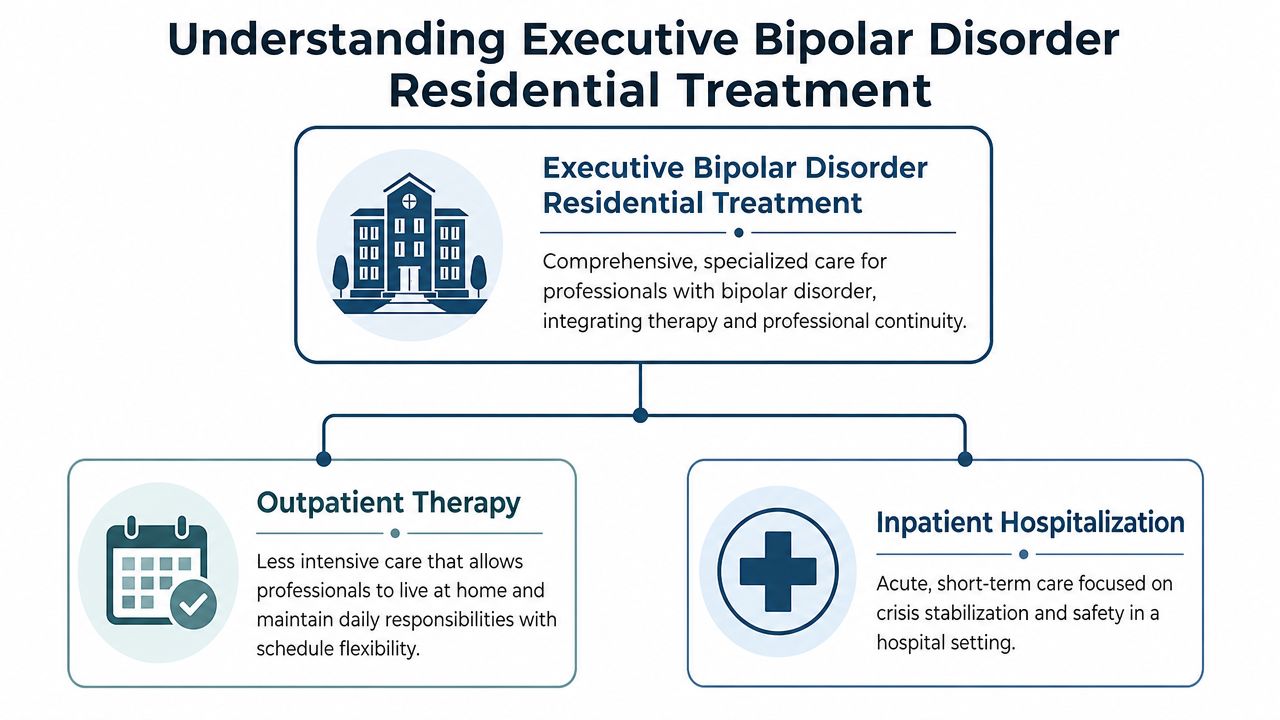
Executive bipolar disorder residential treatment is intensive, structured care in a private, non-hospital setting designed for people who need more than weekly therapy but don't require the restrictions of acute hospitalization. It's especially appropriate when bipolar symptoms are disrupting work, relationships, sleep, or safety, and when a professional needs both clinical depth and discretion.
Bipolar disorder affects an estimated 4.4% of the American population over their lifetime, and effective residential programs for achieving stability often require a minimum stay of six weeks to allow for thorough medication optimization and psychosocial therapy according to lifetime prevalence and residential care guidance from Lindner Center of Hope.
How it differs from the other two common options
A clear comparison helps.
| Level of care | Best use | Limits for executives |
|---|---|---|
| Outpatient therapy | Ongoing support when symptoms are manageable | Often too light when mood instability is escalating |
| Inpatient hospitalization | Acute crisis stabilization and safety | Usually short-term, highly restrictive, and not designed for professional continuity |
| Executive residential treatment | Comprehensive stabilization, therapy, and skill building | Requires a serious time commitment, but that commitment is often what produces real change |
Outpatient care can be useful, but it depends heavily on the person's ability to self-regulate between sessions. During a manic, mixed, or severe depressive phase, that's exactly what starts to fail. Acute hospitalization has an important role, but it's built for immediate containment, not for the deeper work of rebuilding routines, optimizing medication, and addressing the emotional and behavioral patterns that keep episodes cycling.
Why elite treatment is worth the premium
A standard program can offer beds and groups. An elite executive program should offer something more precise: accredited care, expert psychiatric oversight, strong individual therapy, and an environment that treats privacy as a requirement rather than a perk.
The simplest analogy is this. Generic treatment is like attending a crowded seminar when a company is in trouble. Executive residential treatment is like assembling a board of advisors for a problem that could affect the entire enterprise. Bipolar disorder in a high-pressure professional life deserves the second response.
Treatment should fit the stakes. When a career, family, public reputation, and personal safety are all in play, generic care isn't enough.
The best programs also understand that successful professionals don't stop being professionals when they enter treatment. They need protected space to recover, but they also need thoughtful systems that support appropriate contact with the outside world, practical planning, and a respectful level of autonomy.
Clinical Cornerstones of an Elite Program
An elite bipolar residential program earns its price through clinical precision. Executives do not need a polished retreat with generic groups. They need a tightly run treatment model that stabilizes mood, protects cognition, and addresses the exact pressures that come with leadership, visibility, and constant decision-making.
That starts with staffing. A serious program should have psychiatrists, psychologists, primary therapists, and addiction clinicians who know how bipolar disorder presents in high-functioning professionals. Many executives arrive looking productive on the surface while privately cycling through insomnia, irritability, risky judgment, alcohol misuse, panic, or depressive shutdown. If a program mistakes polished performance for stability, treatment will miss the actual illness.
The therapy model also has to fit the patient.
CBT helps identify the thought patterns that turn activation into bad decisions. For an executive, that may mean catching inflated certainty, impulsive spending, aggressive communication, or catastrophic thinking before those patterns damage a company, a marriage, or both.
DBT builds emotional control under pressure. That matters in treatment, and it matters when someone returns to investor calls, board conflict, media exposure, or family stress without escalating into rage, collapse, or self-destructive behavior.
ACT is useful for high achievers who have spent years outrunning distress. It helps patients act from values and judgment instead of fear, ego, exhaustion, or mood state.
Medication work should be equally disciplined. The standard should be clear: reduce mood volatility with the fewest medications necessary, preserve mental sharpness, and monitor closely enough to adjust based on real patterns instead of guesswork. Residential care gives clinicians something outpatient treatment often cannot. Daily observation, consistent sleep data, therapist feedback, and immediate review of side effects.
Research supports that kind of structured care. In the JAMA Psychiatry report on systematic bipolar care, investigators found that structured management and psychotherapy reduced time spent with significant manic symptoms compared with standard care over two years.
For executives, the strongest programs share a few clinical standards:
- A full psychiatric reevaluation: confirm the diagnosis, identify mixed features, review past medication failures, and screen for trauma, anxiety, ADHD, and substance use.
- Daily individual and group treatment: consistency matters more than occasional insight.
- Strict sleep and circadian stabilization: late-night work, travel, and constant device use often keep episodes going.
- Performance-aware treatment planning: therapy should address leadership stress, identity loss, perfectionism, and the pressure to appear fully in control.
- Family or spouse involvement when appropriate: home dynamics can either support recovery or destabilize it.
Programs designed for professionals should also know how to balance intensive treatment with appropriate outside contact. That is one reason families often look for executive-focused luxury residential treatment rather than a standard residential setting that ignores the realities of a demanding career.
One example is Reflections, a California-licensed, Joint Commission-accredited residential provider that offers dual-diagnosis care with PhD-level psychologists, psychiatrists, evidence-based therapies, access to electronics when clinically appropriate, and continuing care planning built around real life after discharge.
Addressing Co-Occurring Conditions and Substance Use
In executive populations, bipolar disorder rarely travels alone. It often arrives with alcohol misuse, stimulant overuse, sedative dependence, anxiety, trauma, or a pattern of self-medication that started as performance management and turned into a second illness. Treating only the mood disorder while ignoring the substance use problem is a setup for relapse. Treating only the addiction while ignoring bipolar disorder is just as weak.
That's why dual-diagnosis care matters. A premium program should treat the whole chain at once: mood instability, career stress, sleep disruption, relationship damage, and the substances used to blunt, boost, or control those states.
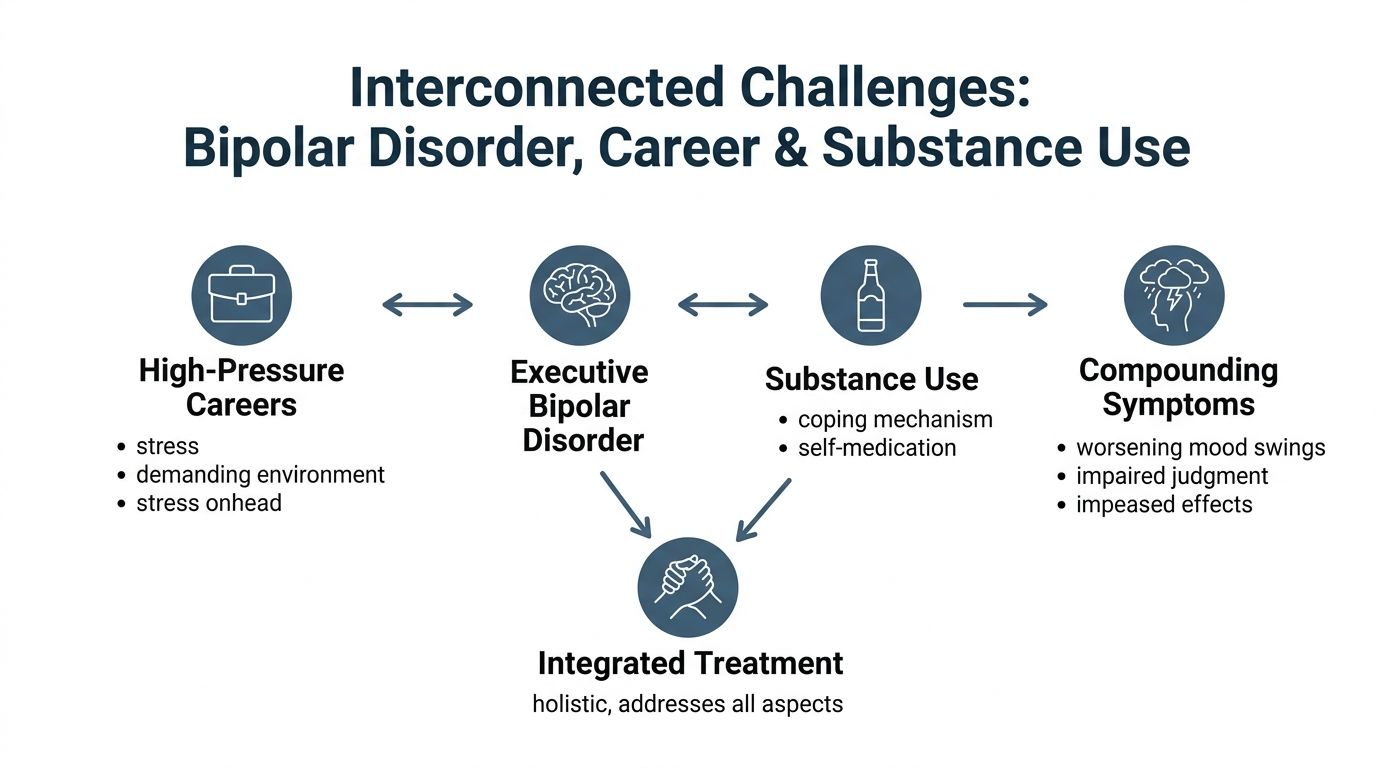
Why professionals get stuck in the cycle
High performers are often rewarded for intensity. That can blur the line between productive drive and destabilizing activation. Then substances enter the picture. Alcohol to slow down. Benzodiazepines to sleep. Stimulants to recover output. Cannabis to “take the edge off.” The short-term logic feels compelling. The long-term effect is usually worse sleep, worse judgment, and more chaotic mood shifts.
For families, this can look baffling. The person is smart, resourced, and highly capable. Yet the pattern keeps repeating because the system around the illness is reinforcing it.
A clear overview of this overlap appears in this explanation of co-occurring disorders, which helps families understand why parallel treatment tracks often fail.
Why detox must protect dignity
When substance use is part of the picture, detox can't be an afterthought. For executives and public-facing professionals, the setting matters. Clinical withdrawal management should be medically supervised, emotionally containing, and private enough that a person doesn't feel stripped of identity at the exact moment they need help most.
Recovery starts faster when the program treats the client like an adult with a serious health condition, not like a disciplinary problem.
A luxury dual-diagnosis setting also removes a common barrier to care. Many professionals delay treatment because they fear humiliation more than symptoms. A discreet residential detox and rehab model answers that concern directly. It allows stabilization in a calm environment while clinicians assess what belongs to withdrawal, what belongs to bipolar disorder, and how the two interact.
The integrated model that works better
Effective care usually includes:
- Sub-acute detox when indicated: medically managed withdrawal with privacy and comfort.
- Psychiatric assessment during early stabilization: symptoms need re-evaluation once substances are no longer distorting the picture.
- Therapy focused on coping and relapse patterns: clients need alternatives to self-medication that fit real work stress.
- Family and systems work: loved ones need practical guidance, not vague encouragement.
For a professional audience, this isn't about moral failure. It's about removing the hidden drivers that keep a brilliant life unstable.
The Residential Experience Privacy and Professional Continuity
The biggest question many professionals ask isn't whether treatment could help. It's whether life outside treatment will collapse while they're gone. In a properly designed executive program, it doesn't have to.
A typical day should feel structured, private, and clinically purposeful. There's time for psychiatry, individual therapy, group work, skills practice, fitness, and quiet recovery. There should also be protected space for appropriate work contact, because many executives cannot vanish for weeks without creating more stress than treatment is meant to reduce.
Why private rooms are non-negotiable
For this clientele, private rooms aren't cosmetic. They're operational. They protect confidentiality, support emotional decompression, and give residents the ability to step away from stimulation when mood regulation is fragile.
In luxury bipolar disorder programs designed for executives, private one-on-one rooms are a standard feature, unlike standard facilities where up to 60% of patients may share rooms, ensuring professionals can maintain dignity and career continuity, as noted in this discussion of executive-focused bipolar treatment settings.
That difference matters. A founder, physician, attorney, or senior executive may need a private conversation with family, counsel, or a trusted colleague. Shared quarters make that harder and less safe.
Why electronics matter in the right hands
Some programs ban phones and laptops outright. For many executives, that policy creates panic, not healing. In a high-end setting designed for working professionals, access to electronics can be clinically managed rather than reflexively prohibited. That approach lets residents maintain essential responsibilities without falling back into nonstop work mode.
A balanced day might include:
- Morning clinical work: psychiatry, medication review, or individual therapy.
- Midday groups and skills practice: DBT, CBT, relapse prevention, or trauma-informed sessions.
- Protected professional window: time-limited access for urgent calls, email review, or strategic decisions.
- Evening regulation practices: fitness, nutrition support, mindfulness, and quiet time.
A thoughtful example of this model appears in luxury rehab for executives, where privacy, electronics access, and clinical structure are treated as compatible rather than contradictory.
The right question isn't “Can a resident keep working?” It's “How can treatment support recovery without creating avoidable professional damage?”
What the environment should feel like
The setting should not feel sterile, punitive, or chaotic. It should feel calm enough for the nervous system to settle and thoughtfully designed so a high-functioning adult doesn't feel infantilized. Nutrition, movement, sleep routines, and mindfulness aren't side benefits in that environment. They're performance restoration tools. A leader who learns to regulate stress, sleep predictably, and respond rather than react leaves treatment stronger than when they arrived.
How to Choose an Accredited Residential Program
A premium price doesn't guarantee premium care. Some centers market luxury and deliver little beyond comfort. For bipolar disorder residential treatment, the standard has to be much higher. Families should vet programs like they would vet a major financial decision. Credentials, structure, and specialization matter more than polished branding.

The non-negotiables
The first filter is accreditation. A program should be able to show that it meets recognized standards for safety, quality, and clinical operations. Families who want a concise explanation should review what Joint Commission accreditation means.
After that, the questions should get sharper.
- Ask about bipolar disorder specifically: many facilities treat mood disorders broadly but don't have depth in bipolar stabilization.
- Ask about dual diagnosis: substance use and mental health must be treated together when both are present.
- Ask who leads care: psychiatric oversight and advanced clinical leadership aren't optional for complex cases.
- Ask about privacy policies: executives need discretion in admissions, treatment participation, and communication.
- Ask about electronics access: a blanket ban may be a poor fit for a working professional with unavoidable obligations.
- Ask about family work and aftercare: treatment that ends at discharge is incomplete.
A quick decision framework
| What to check | What a strong answer sounds like |
|---|---|
| Accreditation | Clear, current accreditation and defined clinical standards |
| Executive focus | The program understands confidentiality, reputation concerns, and work continuity |
| Clinical depth | Evidence-based therapy, psychiatry, medication optimization, and dual-diagnosis capability |
| Living environment | Private rooms, quiet surroundings, and a non-hospital atmosphere |
| Continuing care | A real discharge plan with family support and step-down options |
One more point deserves emphasis. A center should be willing to answer difficult questions directly. If admissions staff dodge questions about staffing, medication practices, or privacy, that's useful information. A serious program doesn't hide behind vague promises.
Investing in Your Future Beyond Treatment
The right residential program doesn't put life on hold. It resets the conditions that make a sustainable life possible. For a successful professional, that means more than symptom relief. It means clearer judgment, steadier relationships, stronger boundaries, and a realistic plan for staying well while carrying responsibility.
That's also why discharge planning matters so much. Residential care that includes vocational and educational instruction, along with coping skills courses, serves as a key milestone in recovery, helping patients rebuild functional independence after their stay, which is critical for long-term success, according to Silver Hill Hospital's description of residential psychiatric care.
What protects the investment after discharge
The strongest programs don't stop at stabilization. They build a bridge back into real life.
- Continuing care planning: psychiatry, therapy, and accountability should already be arranged before discharge.
- Family support: loved ones need guidance on communication, boundaries, and relapse warning signs.
- Vocational reintegration: returning to work should be paced and intentional, not a blind jump back into chaos.
Daily habits matter here too. Recovery becomes more durable when a person can incorporate self-care easily into ordinary routines instead of treating wellness like a separate project.
Seeking treatment is leadership. It's the decision to protect health, career, family, and future before the illness makes another expensive decision on its own.
Reflections offers confidential, accredited residential dual-diagnosis care in California for adults who need specialized treatment in a private setting. For executives, professionals, or families evaluating bipolar disorder residential treatment, Reflections is a practical place to start the conversation.









