Co-occurring disorders, also called dual diagnosis, mean a person has a mental health condition and a substance use disorder at the same time. In the United States, about 8.1 million adults are estimated to have co-occurring disorders, which is more than 40% of people with substance use disorder according to the Recovery Research Institute.
For high-achieving professionals, this often hides in plain sight. The board presentation still lands. The deal still closes. The family still sees someone who appears disciplined and capable. But sleep gets thinner, irritability sharpens, alcohol becomes a nightly tool instead of a choice, or prescription medication shifts from targeted use to quiet dependence.
Co-occurring disorders, or dual diagnosis, is when an individual struggles with both a mental health condition and a substance use disorder at the same time. For executives and other high-functioning professionals, the central problem is rarely lack of intelligence or willpower. It's misidentification. They call it stress, burnout, overwork, or a rough patch. Clinically, it may be something far more specific, and far more treatable.
The High-Functioning Paradox
A senior executive can manage a company crisis by noon, host a client dinner by seven, and still lie awake at two in the morning with racing thoughts and a drink in hand. Outwardly, that life looks controlled. Clinically, it may be deteriorating fast.

The paradox is simple. The more competent a professional appears, the easier it is to miss the warning signs. A leader who never misses deadlines may still be battling depression. A founder who commands a room may be using substances to blunt anxiety before every presentation. A physician, attorney, or C-suite operator may look polished while privately relying on alcohol, stimulants, benzodiazepines, or cannabis to modulate mood, sleep, energy, or confidence.
Success can mask severity
High performers often compensate longer than others. They use intelligence, resources, routine, and image management to delay consequences. That doesn't mean the condition is mild. It usually means the disorder has had more room to entrench itself without obvious public collapse.
Executives rarely seek help when symptoms begin. They seek help when the system that kept them functional stops working.
That's why a precise definition matters. To define co-occurring disorders accurately, one has to look past the stereotype of obvious addiction or obvious psychiatric instability. In practice, these conditions often show up as a pattern of escalating performance strain, emotional volatility, secret relief behaviors, and growing dependence on something that once felt manageable.
Professionals who recognize this pattern often need a treatment setting built for discretion and continuity, not disruption. Programs designed for high-functioning professional addiction treatment are often better suited to the realities of leadership, confidentiality, and career responsibility than generic residential care.
What families often miss
Families usually notice fragments, not the whole picture:
- Mood shifts: More irritability, detachment, or emotional numbness.
- Subtle dependence: More drinking after work, more pills for sleep, more excuses for needing relief.
- Image protection: Strong resistance to help because reputation feels inseparable from survival.
This isn't a character defect. It's a treatable clinical pattern. The mistake is waiting for a public implosion before calling it what it is.
Understanding the Vicious Cycle
A co-occurring disorder doesn't operate like two separate problems sitting side by side. It behaves more like two vines wrapped around the same structure, each tightening the other.
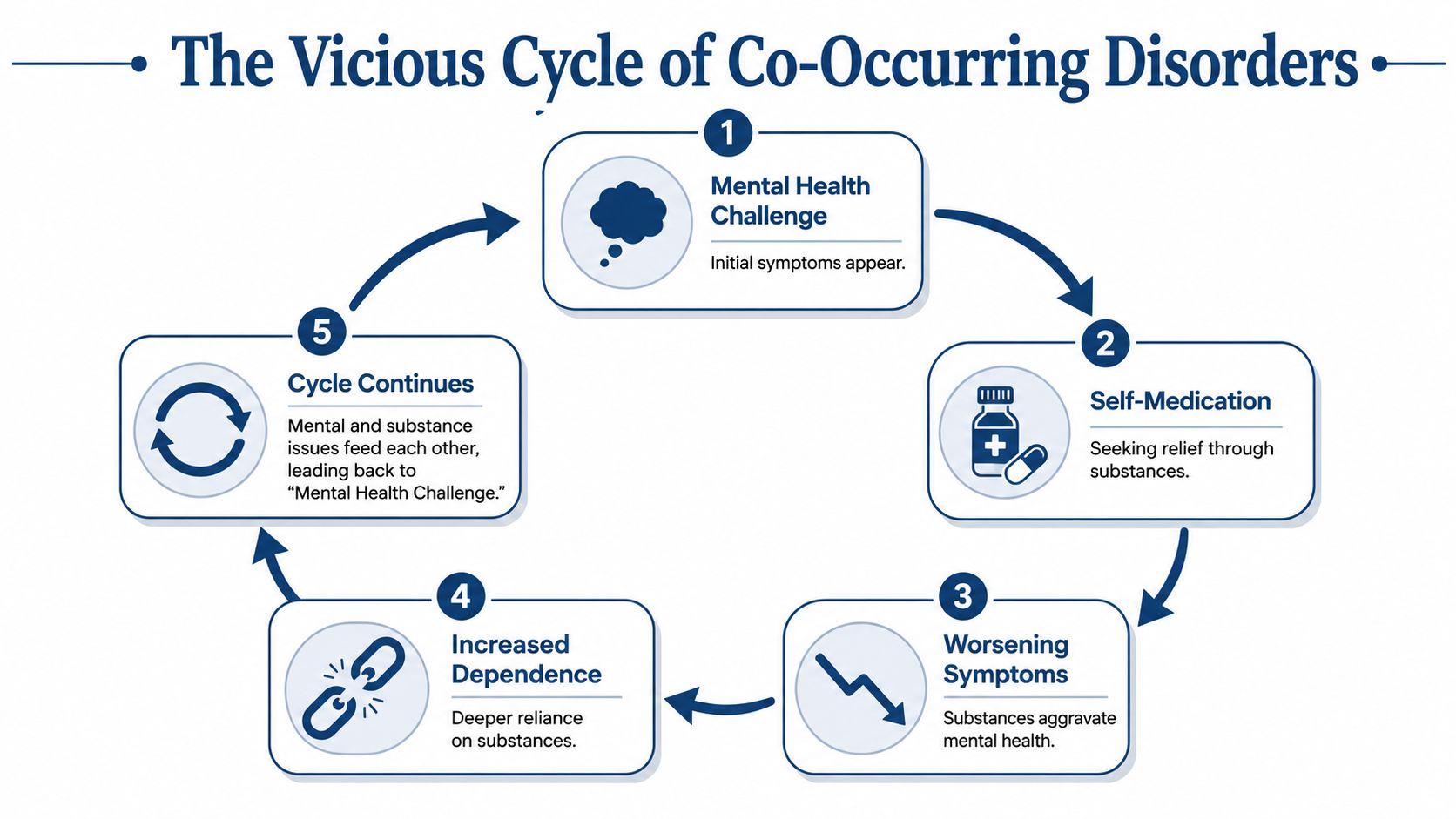
An executive feels anxious, depleted, emotionally flat, ashamed, overstimulated, or unable to sleep. A substance then enters as a solution. Alcohol softens social anxiety. Stimulants override fatigue. Sedatives dampen panic or racing thoughts. Cannabis appears to quiet the mind after relentless pressure. The relief can feel real, especially at first.
Then the second half of the cycle takes hold. Substance use starts to worsen sleep quality, increase emotional reactivity, intensify depression, destabilize concentration, or lower stress tolerance. The professional now feels worse than before, but attributes that decline to work pressure or personal weakness. So the substance use expands.
How the loop usually forms
For professionals, the cycle often follows a recognizable sequence:
- An internal symptom appears. Anxiety, grief, trauma activation, mood instability, insomnia, or burnout starts interfering with daily functioning.
- A performance-preserving workaround develops. The person uses a substance to stay sharp, calm down, sleep, socialize, or push through.
- The workaround becomes structurally important. It no longer feels optional. Meetings, travel, conflict, and recovery from stress start revolving around access to that relief.
- Both conditions become harder to separate. The person can't tell what is causing what. That confusion delays proper care.
Why separate treatment usually fails
Treating only the substance use while ignoring the anxiety, depression, trauma, or bipolar symptoms leaves the driver untouched. Treating only the mental health symptoms while ignoring the drinking or drug use leaves the fuel in place.
Practical rule: If one condition reliably triggers, worsens, or maintains the other, they must be treated together.
Many accomplished people waste time. They try a therapist without addiction treatment. Or they stop drinking without addressing panic, trauma, or despair. Or they take medication while continuing the same pattern of substance use that keeps the psychiatric symptoms unstable.
That approach is inefficient and, for a professional with serious obligations, risky. The right response is a coordinated clinical plan that sees the full loop and interrupts it at every point.
Common Co-Occurring Disorders in Professionals
Among professionals, co-occurring disorders rarely look generic. They often attach themselves to the demands of status, access, travel, responsibility, and relentless performance.
SAMHSA makes an important clarification in its guidance on co-occurring disorders. The term is not limited to one pairing. It can include any combination of two or more substance use disorders and mental disorders. That broader definition matters because many professionals dismiss their symptoms if they don't fit a narrow stereotype.
Patterns often seen in high-pressure lives
A few examples show how this tends to present:
- Anxiety with alcohol use: A professional uses alcohol to take the edge off networking events, travel stress, leadership pressure, or chronic anticipatory tension.
- Depression with stimulant misuse: Someone who feels flat, exhausted, or cognitively slowed leans on stimulants to maintain output and preserve image.
- Trauma-related symptoms with sedative use: A person with intrusive thoughts, hypervigilance, or chronic inner agitation turns to benzodiazepines or other sedating substances for relief.
- ADHD-related difficulties with substance misuse: A leader struggling with focus, impulsivity, disorganization, or overstimulation may overuse substances in an attempt to regulate attention or calm.
- Bipolar symptoms with alcohol or drug use: Mood shifts can be misread as temperament or entrepreneurial intensity while substance use further destabilizes judgment and sleep.
Why executives miss the diagnosis
Professionals often over-intellectualize the pattern. They tell themselves the drinking is “situational,” the stimulant misuse is “temporary,” or the insomnia is the cost of success. That framing protects identity, but it blocks treatment.
A more useful lens is clinical, not moral. If symptoms and substance use are interacting, the problem is no longer a stress-management issue. It's a dual-diagnosis issue.
For families researching treatment models, practical overviews of integrated care for mental health and addiction can help clarify why these pairings need a coordinated response rather than separate referrals.
A polished exterior doesn't rule out serious illness. It often delays recognition of it.
The executive profile adds one more complication. High achievers are often rewarded for intensity, self-containment, and stamina. Those same traits can hide the need for treatment long after the condition has become dangerous.
How Co-Occurring Disorders Are Diagnosed
A proper dual-diagnosis evaluation is not guesswork. It requires a detailed assessment by clinicians who can distinguish between a primary mental health disorder, a substance use disorder, and symptoms caused by intoxication or withdrawal.
That distinction is where mediocre treatment often fails. A person can appear depressed during withdrawal, anxious during stimulant use, or emotionally unstable during chronic sleep disruption and heavy substance exposure. If a program labels those symptoms too quickly, treatment goes off course.
What a real assessment looks for
Clinicians need to answer several questions:
- What substances are being used, and how often?
- When did the psychiatric symptoms begin?
- Did the mental health symptoms exist before heavy substance use, or did they emerge during it?
- What happens to those symptoms after stabilization?
- What family, medical, occupational, and trauma history shapes the picture?
A serious assessment also looks at function, not just symptoms. For professionals, that means examining changes in judgment, executive functioning, sleep, interpersonal behavior, risk-taking, and hidden deterioration behind continued achievement.
The key diagnostic distinction
For a true co-occurring diagnosis, psychiatric symptoms must persist for 4 to 6 weeks after acute intoxication or withdrawal ends, ruling out a transient substance-induced disorder. This distinction is critical because treating only one condition yields a 70 to 80% relapse rate within 12 months.
That is why rushed admissions, superficial intake interviews, and one-size-fits-all labels are unacceptable for this population. Executives often present with complex symptom pictures, polished defenses, and intense pressure to minimize. The clinical team has to be able to see through all three.
The first job of treatment is diagnostic clarity. Without it, even motivated patients can spend months working hard on the wrong problem.
What professionals should demand
A high-level program should provide:
| Clinical requirement | Why it matters |
|---|---|
| Multidisciplinary evaluation | Mental health and addiction symptoms need coordinated review, not isolated opinions. |
| Psychiatric oversight | Medication decisions have to account for substance history and current stabilization. |
| Psychological depth | Trauma, mood disorders, anxiety, and personality patterns can complicate presentation. |
| Time for observation | Some diagnoses only become clear after the nervous system settles. |
For executives, this process should also be discreet. Privacy isn't a luxury item in this setting. It is part of effective care, because honest disclosure only happens when the person feels professionally protected.
The Power of Integrated Dual-Diagnosis Treatment
Once the diagnosis is clear, the treatment model matters as much as the diagnosis itself. Fragmented care is common, and it's a poor fit for co-occurring disorders.
A professional may see one clinician for anxiety, another for addiction, and a prescriber who only sees part of the picture. Each provider may be competent. The system is still flawed because the conditions are interacting continuously.
Fragmented care versus integrated care
Here's the practical difference:
| Model | What happens |
|---|---|
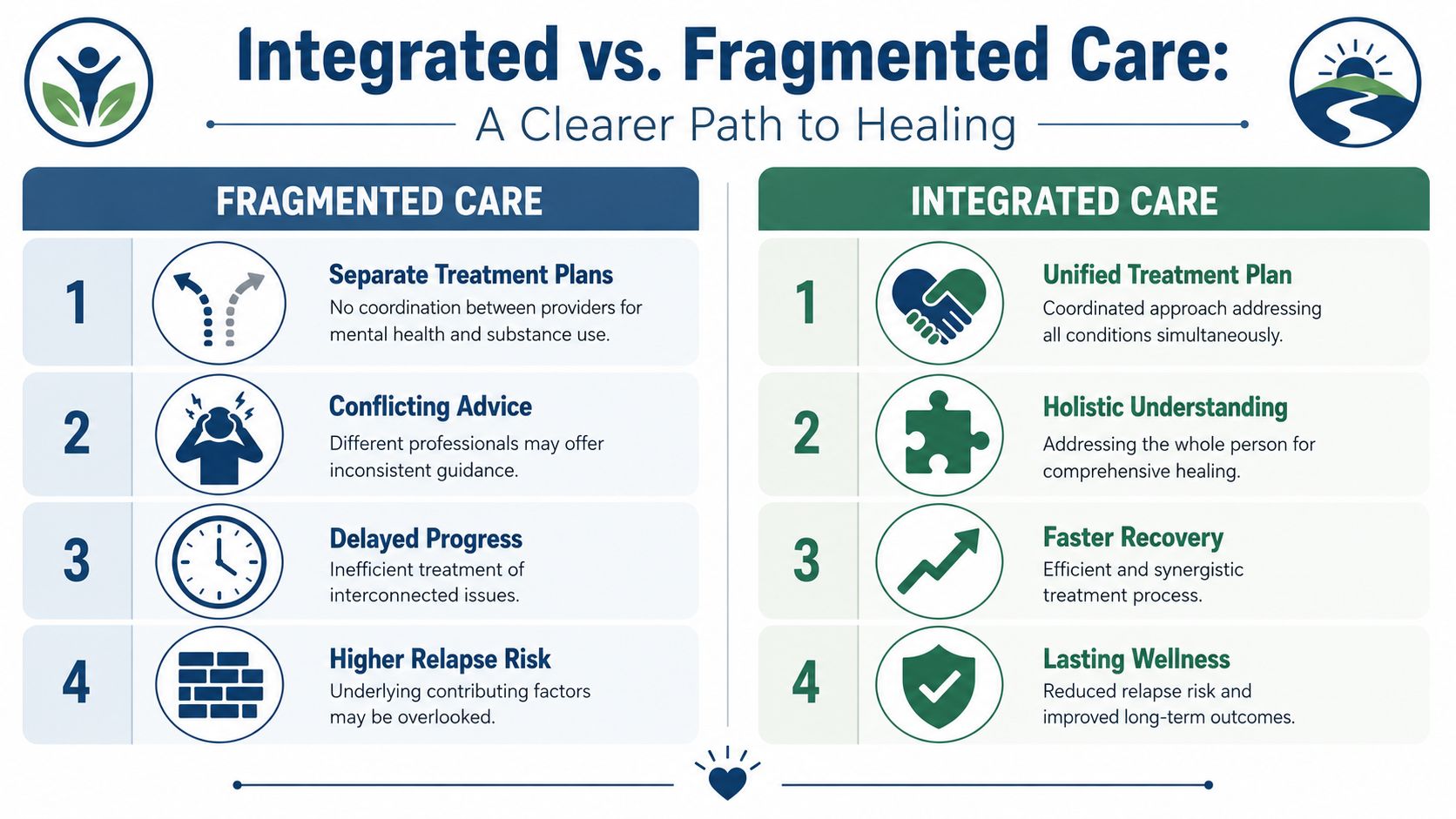
| Fragmented care | Mental health and substance use are treated separately, often with inconsistent goals and incomplete communication. |
| Integrated care | One coordinated team treats both conditions at the same time with a unified plan. |
Failure to provide integrated care results in fragmented care, which correlates with higher hospitalization rates, increased mortality, and a 60% reduction in treatment retention compared to integrated models.
That outcome makes sense clinically. If anxiety triggers drinking, and drinking worsens anxiety, then splitting treatment into separate silos forces the patient to manage a connected illness through disconnected systems.
What integrated treatment actually includes
An effective dual-diagnosis program usually combines several elements at once:
- Unified treatment planning: One team tracks the interaction between symptoms, substance use, sleep, medication response, and behavior.
- Specialized therapy for dual diagnosis: Approaches such as CBT and DBT are adapted to address both emotional regulation and substance patterns together.
- Medication management with context: Prescribing decisions take addiction risk, withdrawal history, and psychiatric need into account.
- Family involvement when appropriate: Families learn how to support recovery without enabling secrecy, minimization, or chaos.
For readers who want an additional outside perspective on understanding co-occurring conditions, it can be useful to compare how integrated models frame the problem as one interconnected clinical system.
A focused internal overview of integrated mental health and addiction treatment also helps clarify what coordinated care should look like in practice for complex presentations.
Treating one half of a co-occurring disorder is like repairing one side of a bridge while the other side keeps collapsing.
For executives, integrated care is not only more evidence-based. It is more efficient. It reduces mixed messages, shortens the path to diagnostic precision, and gives the patient one coherent roadmap instead of several conflicting ones.
Choosing Treatment Without Sacrificing Your Career
The usual objection from executives isn't whether treatment would help. It's whether treatment can happen without destroying momentum, confidentiality, or credibility.
That concern is legitimate. A generic program that treats every resident the same way is often a poor match for a person with fiduciary duties, leadership visibility, family obligations, and a constant flow of sensitive communication.

Non-negotiables for high-level professionals
A treatment setting for this population should include:
- Private accommodations: Private rooms in detox and residential care protect dignity, sleep, and discretion.
- Access to electronics when clinically appropriate: Many professionals need structured access to laptops and phones to manage essential responsibilities.
- Clinical depth: The team should be able to handle trauma, mood disorders, anxiety, substance dependence, and executive-level resistance in the same case.
- Confidentiality baked into operations: Privacy has to be operational, not merely promised.
- Peer fit: Professionals often do better around others who understand the pressures of leadership, image, and high accountability.
What to avoid
Some programs frame total disconnection as the only serious path to recovery. That may work for some patients. It is not universally necessary, and for many executives it becomes a reason to delay treatment until the situation worsens.
The better question is whether the program can balance recovery with reality. For some patients, that means limited, structured work contact. For others, it means stepping back more fully for a defined period. Good clinical care individualizes that decision.
Reflections is one example of a program built for this intersection of privacy, dual-diagnosis care, private accommodations, and appropriate access to electronics for clients who need to remain engaged with work while receiving treatment.
Professionals comparing options often start with dedicated programs for treatment centers for working professionals, because career continuity and clinical rigor should be planned together, not forced into conflict.
The right program protects recovery first, while also respecting the practical realities of leadership and reputation.
A career doesn't have to be sacrificed for treatment. But the treatment setting must be chosen with the same precision that a serious executive brings to any high-stakes decision.
FAQs for Professionals Considering Treatment
Will treatment remain private?
It should. Professionals need a setting where confidentiality is strict, communication is controlled, and disclosure is never casual. A discreet program will protect personal information, keep the environment private, and create space for honest treatment without unnecessary professional exposure.
Privacy also improves assessment quality. When patients don't fear reputational fallout, they disclose more accurately.
Can family be involved without creating more chaos?
Yes, if the program structures it correctly. Family involvement works best when it is guided by clinicians, not improvised in the middle of a crisis.
That usually means a combination of private family sessions, psychoeducation, boundary work, and practical planning around communication, support, and post-treatment expectations. Families often need help understanding the disorder without becoming the compliance department.
What happens after residential treatment?
Strong programs don't treat discharge as the end of care. They build continuing care, alumni support, outpatient planning, and relapse-prevention structure into the transition.
For professionals, aftercare should also account for travel, leadership stress, social obligations, and the pressure to “get back to normal” too quickly. Recovery usually holds better when re-entry is deliberate.
Why act now instead of waiting?
Because delay is common, and it's costly. In 2022, about 21.5 million U.S. adults had both a mental illness and a substance use disorder, yet only 10% received treatment for both conditions, while 42% received no treatment at all, according to the National Institute on Drug Abuse.
That gap says something important. Many people know they're struggling. Far fewer get the right level of care.
For executives and families, the practical standard should be simple:
- Choose diagnostic precision over reassurance
- Choose integrated treatment over fragmented referrals
- Choose privacy that is operational, not cosmetic
- Choose a setting that can accommodate professional realities without minimizing the illness
For professionals and families seeking discreet, clinically advanced dual-diagnosis care, Reflections offers private residential treatment designed for adults who need serious help without unnecessary disruption to career and family responsibilities.








