A private thought tends to arrive before any phone call does. A senior executive closes the office door, looks at the calendar, and realizes that drinking is no longer a background habit. It has become part of how the day starts, how stress is blunted, and how sleep is forced. The fear isn't only about stopping. The fear is about what happens if stopping goes badly.
For high-profile professionals, that fear is layered. There's concern about safety, concern about privacy, and concern about whether stepping into care means disappearing from obligations at the exact moment life feels least able to pause. Many people in this position have spent years solving complex problems quickly. Alcohol withdrawal is different. It doesn't reward improvisation.
That's why alcohol withdrawal management should be approached as a confidential medical process, not a personal endurance test. For executives and working professionals, the right setting protects more than physical stability. It protects judgment, reputation, and continuity.
Navigating Alcohol Withdrawal with Executive Care
A common scenario is easy to recognize. A founder or physician leader has tried to cut back at home over a long weekend. By evening, hands begin to shake. Sleep doesn't come. Anxiety rises fast, then faster. The next morning brings meetings, family expectations, and a private sense that this may no longer be manageable alone.
For professionals used to control, withdrawal can feel uniquely destabilizing. The loss of predictability is often more frightening than the symptoms themselves. Many worry that entering treatment means surrendering privacy, losing access to communication, or stepping into a generic environment that doesn't understand the realities of executive life.
What executive-level care changes
A clinically managed, private detox setting answers those concerns directly. The standard isn't solely abstinence. The standard is safe stabilization with discretion.
That means care is organized around several realities:
- Privacy matters clinically and personally: High-visibility clients often delay treatment because they fear exposure more than illness.
- Comfort affects compliance: A private room, calm environment, and respectful staffing reduce friction during an already stressful process.
- Continuity matters: When clinically appropriate, access to phones and laptops can allow a resident to maintain essential communication without turning treatment into a public disruption.
- Sophistication matters: A discerning client usually responds well when the process is explained clearly, decisions are justified, and care feels precise rather than formulaic.
Withdrawal management should feel contained, orderly, and medically intelligent. Chaos has no therapeutic value.
Why this first step matters
Withdrawal isn't the whole of recovery, but it is the point where many people either enter real treatment or retreat back into dangerous self-management. In a high-end clinical setting, the process is designed to lower risk while preserving dignity. That combination often makes the difference between a stalled intention and an actual start.
For executives, the right withdrawal program doesn't ask them to choose between health and identity. It creates a setting where both can be protected while the body safely comes off alcohol.
The Clinical Realities of Alcohol Withdrawal
A common executive mistake is to judge withdrawal by the first few hours. Someone stops drinking after a week of heavy evening use, wakes at 3 a.m. sweating, shaky, and unable to sleep, then assumes it is anxiety or exhaustion. By the time blood pressure climbs, tremor worsens, and thinking becomes less clear, the situation has already moved beyond what self-management handles well.
Alcohol withdrawal is a neurophysiologic rebound. Repeated alcohol exposure slows central nervous system activity over time, and the brain adapts to that suppression. Once alcohol is removed, that adaptation remains in place for a period, so the nervous system becomes overactive instead of returning immediately to baseline. Clinicians describe that state as hyperexcitability, and it explains why symptoms can range from restlessness and insomnia to seizures, hallucinations, and delirium.
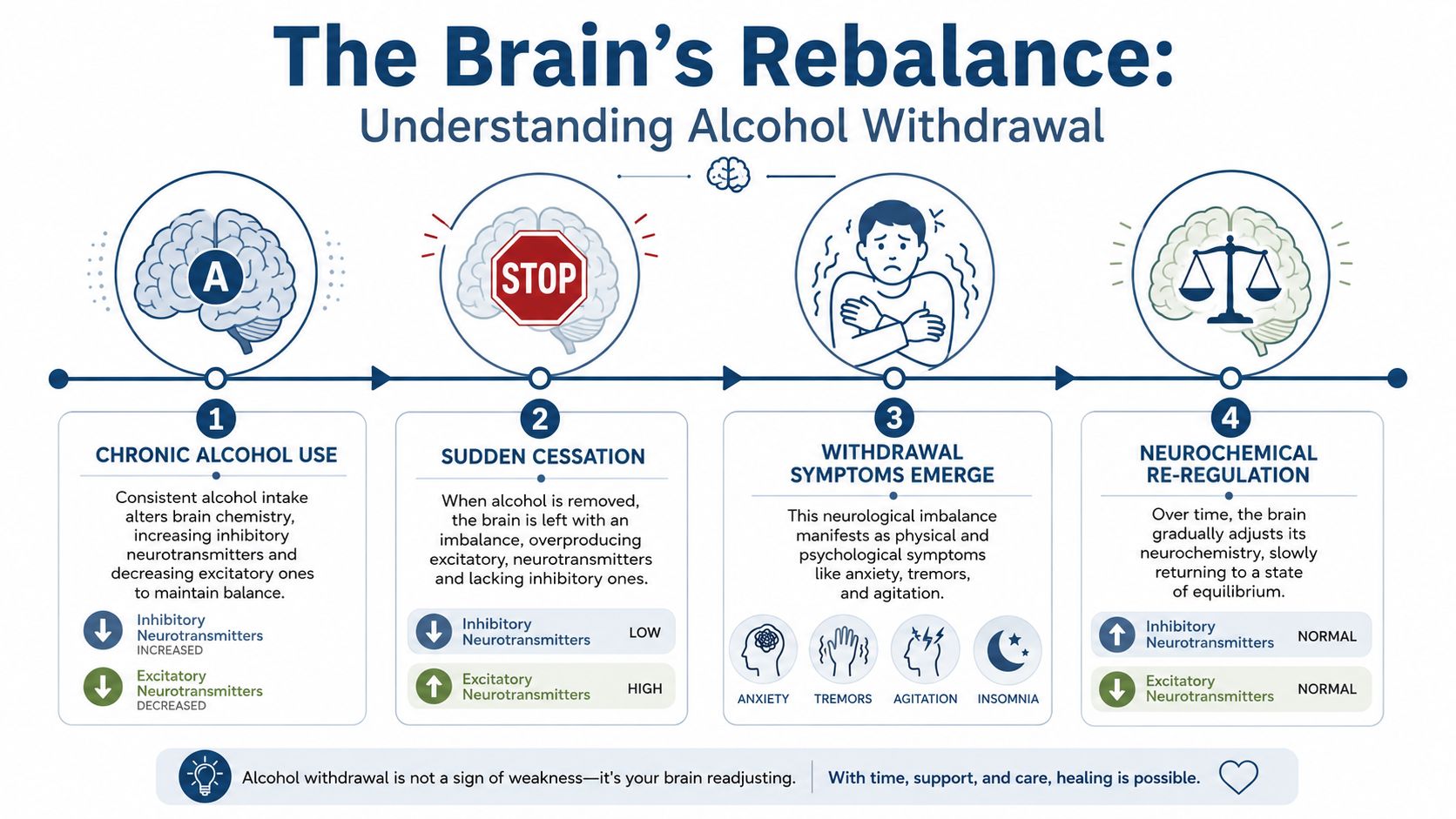
The timeline matters because risk is front-loaded. The National Institute on Alcohol Abuse and Alcoholism notes that symptoms can begin within hours after stopping alcohol, usually peak within the first day or two, and may progress to severe complications such as seizures or delirium tremens during the early withdrawal period in some patients, as described in NIAAA's overview of alcohol withdrawal syndrome. In practice, that means the first 48 to 72 hours deserve the closest observation, especially for people with a long drinking history, prior detox attempts, or medical illness.
For executives and public-facing professionals, that early window creates a specific problem. The body may be medically unstable at the exact moment the person is trying to preserve judgment, confidentiality, and professional continuity. A private, structured setting is designed for that reality, not just for symptom control. This overview of a private professional approach to alcohol detox explains how monitored care protects both safety and discretion.
Symptoms often build in sequence, but not always neatly. Mild early signs can look manageable until they are not.
- Autonomic activation: tremor, sweating, rapid pulse, increased blood pressure
- Psychological and cognitive strain: anxiety, irritability, poor concentration, insomnia
- Physical distress: nausea, headache, loss of appetite, sensitivity to light and sound
- Escalation signs: worsening confusion, perceptual disturbance, severe agitation, seizure activity
That variability is why experienced teams do not rely on appearance alone. A person can look composed, answer emails, and still be developing clinically significant withdrawal.
| Phase | What clinicians watch for |
|---|---|
| Early hours | tremor, anxiety, sweating, insomnia |
| Peak window | worsening agitation, confusion, seizure risk |
| Recovery phase | stabilization, nutrition, hydration, sleep restoration |
Severe withdrawal is not the majority outcome, but it is serious enough that prediction by willpower, professional status, or prior productivity is unreliable. In a medically managed program, the goal is straightforward. Detect deterioration early, treat it promptly, and keep the process quiet, controlled, and clinically precise.
How Clinicians Evaluate Your Need for Care
Good withdrawal care starts with sorting risk, not making assumptions. Two people can both say they “drink too much” and require very different levels of support. One may be appropriate for close ambulatory management. Another may need residential or hospital-based monitoring from the outset.
Risk stratification comes first
Major guidance from ASAM and WHO recommends inpatient management for patients at higher risk of severe withdrawal, including those with prior complicated withdrawal, seizures, delirium, or significant medical or psychiatric comorbidities, as outlined in the ASAM alcohol withdrawal management guideline.
That principle sounds simple, but in practice it's detailed. Clinicians don't just ask how much someone drinks. They examine the pattern and context of use, prior attempts to stop, medical history, current medications, psychiatric symptoms, and whether the person has reliable support outside a supervised setting.
What the assessment usually includes
A rigorous intake often looks at several domains at once:
- Withdrawal history: prior seizures, confusion, hallucinations, or previous detox episodes that became difficult
- Current symptom burden: visible tremor, sweating, agitation, insomnia, nausea, blood pressure changes, and mental status
- Coexisting conditions: liver concerns, cardiovascular issues, panic symptoms, depression, trauma history, or unstable mood states
- Environmental safety: whether the home setting is calm, supported, and medically reachable if symptoms worsen
SA Health notes that the CIWA-Ar scale is commonly used to track withdrawal severity. It gives clinicians a structured way to measure symptoms rather than relying on rough impressions. In an executive setting, that objectivity matters. Discerning clients usually want to know that medication decisions are tied to observed severity, not guesswork.
Why one-size-fits-all detox fails
A fixed plan can miss what matters most. Some patients become more symptomatic quickly and need faster medication adjustment. Others are more vulnerable to oversedation and need tighter clinical judgment.
Clinical rule: The safest plan is the one that matches predicted severity, not the one that sounds most convenient.
This is also where a premium residential environment becomes clinically relevant, not merely comfortable. Privacy, continuous reassessment, and immediate escalation capacity allow the treatment team to respond in real time. For a professional whose work depends on cognitive performance and discretion, that precision is the difference between being looked after and being managed loosely.
The Gold Standard in Medication-Assisted Withdrawal
The strongest medical argument for supervised withdrawal is straightforward. Withdrawal symptoms can worsen quickly, and the most effective treatment is usually time-sensitive. A clinically managed setting allows medication to be adjusted based on actual symptom intensity while nursing staff and prescribing clinicians monitor the whole picture.

Why benzodiazepines remain first line
The World Health Organization recommends benzodiazepines as the first-line medication for alcohol withdrawal management, generally for the first 3 to 7 days after alcohol cessation, according to WHO guidance on management of alcohol withdrawal.
In well-run programs, these medications aren't given casually. The point is to reduce the hyperexcitable withdrawal state early enough to lower risk and improve comfort. Many teams prefer symptom-triggered treatment when appropriate because it aligns medication with the actual severity of withdrawal rather than automatically medicating on a rigid schedule.
That matters for executives who are worried about feeling heavily sedated. The goal isn't to flatten a person. The goal is controlled stabilization.
For readers who want a broader clinical overview of this treatment category, medication-assisted treatment in rehab offers useful context.
Supportive care isn't secondary
Medication is only one part of high-level alcohol withdrawal management. Good care also includes nutrition, hydration, monitoring, and neurological protection.
WHO also recommends:
- Oral thiamine for all patients
- Parenteral thiamine for those at high risk of Wernicke's encephalopathy
- More intensive parenteral thiamine treatment when Wernicke's is suspected
These details matter because alcohol use often affects nutrition long before someone enters treatment. Repletion isn't cosmetic. It's part of preventing avoidable complications.
What premium clinical care actually looks like
A luxury detox program shouldn't mean softer medicine. It should mean better-delivered medicine.
That often includes:
- Private observation in a calm room: less stimulation, better rest, more honest symptom reporting
- Frequent reassessment: vital signs, symptom scores, orientation, hydration status, and sleep
- Minimal effective pharmacology: enough medication to protect safety and reduce suffering, without reflexive overmedication
- Discreet coordination: physicians, nurses, therapists, and psychiatric staff working from the same clinical picture
One example is Reflections, which offers clinically managed medication-assisted withdrawal within a private residential setting for adults who need supervised detox alongside broader mental health and addiction care.
The best detox protocol is rarely the most dramatic one. It's the one that stays ahead of symptoms without clouding the person unnecessarily.
That approach is especially relevant for high-functioning professionals. They usually don't need theatrics. They need competent medicine, privacy, and a team that understands the cost of getting either wrong.
Choosing the Right Level of Care for Your Career
Executives often ask a practical question first. Can withdrawal be handled while staying at home and keeping the workday mostly intact? Sometimes, in carefully selected low-risk cases, the answer can be yes. But that answer depends on real clinical criteria, not preference alone.
Outpatient versus residential in real life
Expert sources emphasize that effective outpatient withdrawal management requires intensive follow-up and that the transition plan into ongoing care often drives success, as discussed in this Curbsiders review of outpatient alcohol withdrawal management.
That point is frequently missed. Outpatient care can sound efficient because it seems less disruptive. For a busy executive, though, the hidden demands are substantial. Symptoms must be reassessed closely. Escalation decisions must happen quickly. The home environment must stay stable, low-trigger, and supported.
A strategic comparison
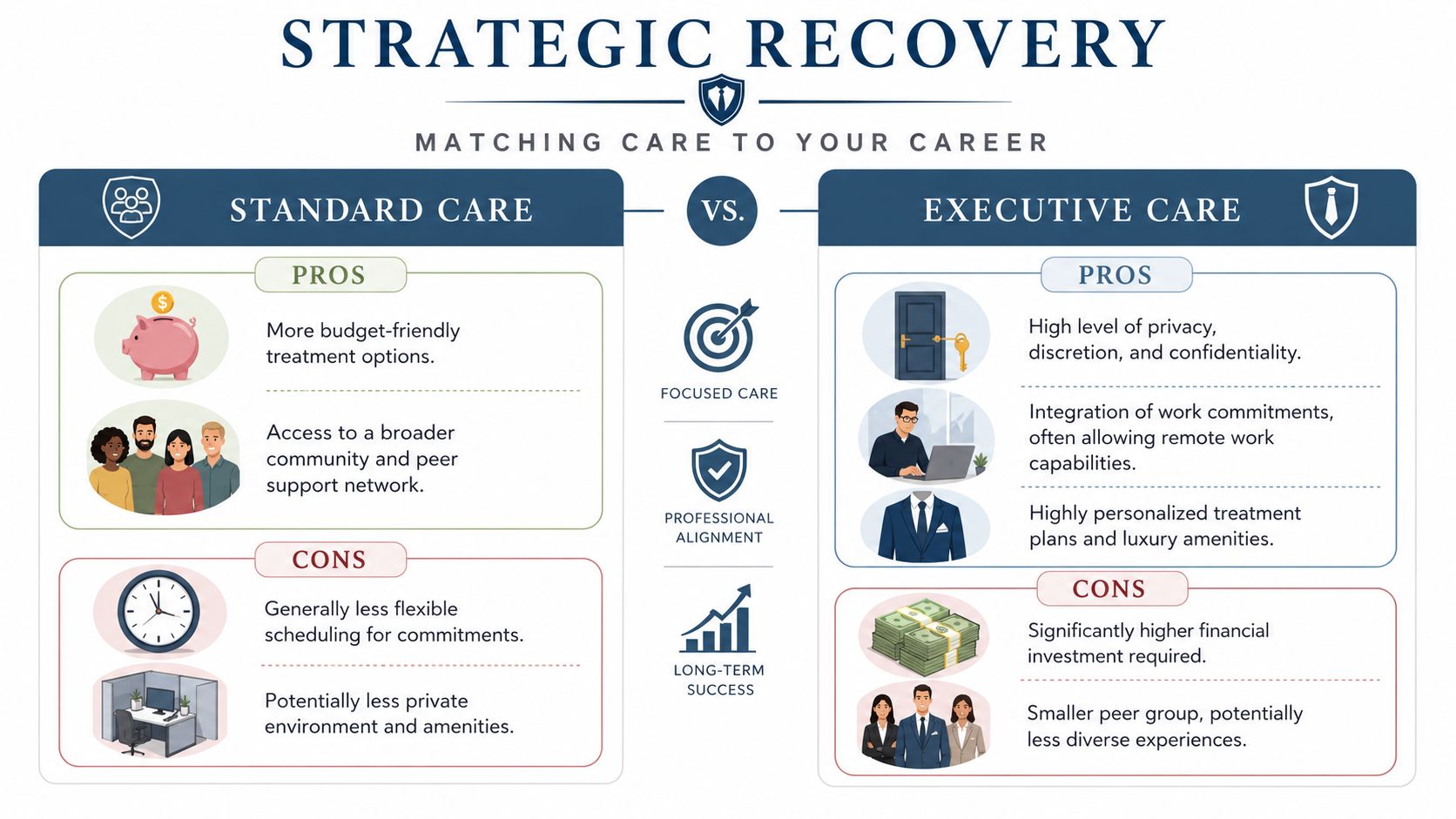
| Setting | Strengths | Trade-offs for professionals |
|---|---|---|
| Outpatient withdrawal care | More flexibility, less visible disruption | Requires reliable support, close follow-up, and a safe home setting |
| Residential executive care | Continuous monitoring, privacy, controlled environment, integrated step-down planning | Greater financial commitment and a formal pause from normal routine |
For many high-achieving clients, the residential option is the more career-protective choice. It removes triggers, reduces the chance of an avoidable emergency, and creates a discreet buffer around a period when judgment and physiology may be unstable.
A useful overview of inpatient versus outpatient rehab considerations can help frame that decision in practical terms.
Work continuity matters, but safety decides
Executive care should acknowledge reality. Some clients need secure access to email, scheduled calls, or selective laptop use because completely disappearing would create larger personal and professional consequences. In a well-structured residential setting, that access can be built in when clinically appropriate, rather than treated as a forbidden luxury.
At the same time, treatment shouldn't become a dressed-up co-working space. The clinical team has to judge when work engagement supports stability and when it interferes with it. The right program keeps health in charge of the schedule.
Professionals who are already reflecting on overextension often find value in broader material on balance and burnout, including WeekdayDoc resources for balanced careers. The appeal isn't lifestyle branding. It's the recognition that sustained recovery usually requires changes in workload, boundaries, and stress response, not just a successful detox.
A private residential program often gives professionals something outpatient care can't. Space to recover without performing normalcy while their nervous system is still unsettled.
For executives, that's often the deciding factor. The most efficient option on paper isn't always the safest or most discreet option in practice.
Managing Withdrawal with Co-Occurring Conditions
Alcohol withdrawal rarely arrives alone. Many professionals who seek care are also carrying untreated or partially treated anxiety, depression, trauma, chronic insomnia, or unstable mood symptoms. Those conditions can complicate withdrawal in ways that aren't obvious at first glance.
When symptoms overlap
The overlap creates two clinical problems. First, pre-existing psychiatric symptoms can intensify the distress of withdrawal. A person with panic may experience early withdrawal as overwhelming and lose confidence quickly. A person with depression may enter detox already depleted, hopeless, and physically neglected.
Second, acute withdrawal can temporarily amplify underlying mental health symptoms. Anxiety may spike. Sleep can collapse. Trauma-related hyperarousal can become harder to distinguish from the autonomic symptoms of withdrawal. Irritability and agitation may look behavioral when they are neurochemical, psychiatric, or both.
Why integrated treatment matters from day one
Dual-diagnosis capability is essential. A high-functioning attorney with alcohol dependence and untreated PTSD doesn't need addiction care first and mental health care later. That split often misses the reason alcohol became functional in the first place.
Integrated teams look at questions such as:
- What is withdrawal, and what is baseline psychiatric distress?
- Which medications relieve symptoms safely, and which may worsen mood, cognition, or sleep afterward?
- What coping pattern has alcohol been covering over?
- What needs to begin immediately so detox doesn't become a brief interruption followed by relapse?
The most successful withdrawal management plans treat alcohol dependence and mental health symptoms as interacting problems, not separate tracks.
That approach is especially important for executives because high performance can hide impairment for a long time. A person may still be meeting deadlines while privately using alcohol to manage dread, racing thoughts, shame, or traumatic activation. Once alcohol is removed, those drivers often come into view rapidly.
The clinical advantage of one coordinated team
In an integrated residential setting, psychiatrists, psychologists, therapists, and addiction clinicians can assess the same person at the same time. That reduces fragmentation. It also improves precision. A treatment team can tell whether worsening insomnia is part of withdrawal, a trauma response, a mood disorder, or some combination.
For the client, the benefit is practical. They don't have to perform their story repeatedly for disconnected providers. They don't have to choose between treating the drinking and treating the reason they've been relying on it. Both can begin together, which creates a much stronger base for recovery after withdrawal ends.
Your Next Step Toward Safe and Lasting Recovery
At 2 a.m., the question is rarely whether drinking has become a problem. The question is whether stopping tonight is safe, private, and realistic, especially if tomorrow still includes a board call, a family obligation, or public visibility. For executives and other high-profile clients, that decision deserves medical judgment, not guesswork.
Residential withdrawal care is the right next step when the medical risk is meaningful, the home setting is unreliable, or prior attempts to stop have become unstable. I tell clients the same thing every day. The goal isn't limited to navigating a challenging week. The goal is to come through withdrawal with judgment intact, health protected, and a treatment plan that fits real life.
Red flags that call for residential medical supervision
A prompt confidential assessment is appropriate if any of the following are true:
- Prior complicated withdrawal: any history of seizures, delirium, hallucinations, or a previous detox that worsened quickly
- Heavy or sustained alcohol use: especially if alcohol is being used to steady hands, control anxiety, sleep, or function during the workday
- Co-occurring medical or psychiatric concerns: depression, panic, trauma symptoms, bipolar features, high blood pressure, liver concerns, or other medical instability
- Limited support at home: living alone, inconsistent supervision, easy access to alcohol, or no reliable person available if symptoms intensify
- High need for discretion: public visibility, senior leadership responsibilities, or family and legal complexity that make a failed home detox costly in more than one way
What an effective next move looks like
The first call should answer practical questions quickly. How severe is the withdrawal risk? What level of care is appropriate? Which medications are likely to help? Can treatment safely accommodate limited work access without undermining recovery?
Those details matter because detox is a starting point, not a stand-alone solution. Long-term recovery outcomes are stronger when withdrawal management connects directly to ongoing treatment and mutual-support or recovery support involvement, as summarized by the National Institute on Alcohol Abuse and Alcoholism in its guidance on treatment approaches for alcohol use disorder. Without that follow-through, many people complete detox, feel briefly better, and return to the same pressures, same triggers, and same drinking pattern.
A medically advanced residential program offers more than observation. It provides physician oversight, psychiatric input when mood or sleep symptoms complicate the picture, nursing support, medication adjustments, nutrition, and a setting designed to reduce exposure and interruption. For a client who must protect privacy and still maintain some continuity with professional obligations, that structure can make treatment both safer and more workable.
For professionals who need confidential, clinically managed alcohol withdrawal care with private rooms, dual-diagnosis treatment, and appropriate access to electronics during treatment, Reflections provides a California-licensed residential option where medical stabilization can connect directly into ongoing recovery planning.









