A managing partner closes another quarter with numbers that look strong on paper, yet mornings now start with a drink, a pill, or both. Sleep is uneven. Temper is shorter. Family members have begun adjusting around the problem. Colleagues may not know the full story, but they can feel the volatility.
For high-achieving professionals, this decision rarely feels like a simple health choice. It feels like a referendum on identity, privacy, and control. The question isn't only whether treatment is needed. The question is which level of care protects long-term judgment, leadership capacity, family stability, and reputation.
That's why the inpatient vs outpatient rehab decision has to be made strategically. An executive with co-occurring anxiety, trauma, depression, or burnout often needs more than a schedule of appointments. At the same time, stepping away from work completely may feel unrealistic, especially when teams, boards, clients, or investors still expect responsiveness.
Luxury treatment exists for this exact intersection of needs. The right program treats substance use and mental health with depth, while also respecting discretion, professional obligations, and the reality that some clients cannot easily disappear. For readers evaluating whether executive rehab can support professional life without sacrificing treatment quality, the central issue is fit. The wrong level of care wastes time. The right one restores stability before the damage becomes harder to contain.
The Executive's Crossroads Choosing the Right Path to Recovery
The executive profile often hides severity well.
A senior attorney may still bill at a high level while privately cycling between alcohol, sleep medication, and panic. A founder may continue raising capital while becoming increasingly dependent on stimulants by day and sedatives by night. A physician or finance professional may maintain outward precision long after internal control has started to erode.
Why this choice carries different stakes
Professionals in visible roles usually delay treatment for three reasons:
- Confidentiality concerns: They worry about who will know, what will be documented, and how absence will be interpreted.
- Career continuity: They assume effective treatment requires total disconnection from work.
- Complex clinical needs: They often have layered presentations, including substance use alongside anxiety, depression, trauma, grief, or chronic stress.
Those concerns are legitimate. They shouldn't be minimized.
The wrong program for an executive is often the one that treats addiction in isolation and ignores the professional ecosystem the client must eventually return to.
What a strategic decision looks like
A strategic decision starts with acuity, not convenience. If withdrawal risk is significant, if relapse has become repetitive, if home has become a trigger-rich environment, or if psychiatric symptoms are intensifying, a more contained setting usually makes sense. If symptoms are milder, home is stable, and the person can reliably engage in treatment while staying accountable, outpatient care may be workable.
For high-performing clients, the best decision often comes from asking a different question: which setting gives this person the highest chance of fully engaging, completing treatment, and returning to life with steadier judgment than before.
Understanding the Spectrum of Care for Professionals
Professionals rarely choose between two simple options. They are choosing how much structure they need, how much risk is present outside treatment, and whether their current routine supports recovery or keeps the problem in motion.
Residential care and why containment matters
The clearest difference between inpatient and outpatient treatment is containment. Inpatient care places the client in a residential setting with continuous supervision, while outpatient treatment allows the person to remain at home and attend scheduled clinical sessions, as described in this overview of inpatient and outpatient treatment levels.
For a high-achieving professional, that difference has practical consequences. A residential setting protects time, attention, sleep, and clinical focus. It also reduces exposure to the specific pressures that often keep substance use going, including constant communication, easy access to alcohol or drugs, strained relationships, and a work culture that rewards endurance over honesty.
I often tell clients to judge level of care by one question. How much of your day needs to be protected for treatment to work?
Residential care usually makes more sense when the answer is, most of it.
Outpatient levels and what they mean for a working schedule
Outpatient treatment covers several levels of care, and the distinctions matter for professionals trying to preserve select responsibilities without undermining treatment.
- Partial Hospitalization Program: This is the most time-intensive outpatient option and can occupy much of the day on most weekdays. It may suit someone who needs strong clinical support but does not require overnight care.
- Intensive Outpatient Program: This level offers a meaningful treatment schedule across the week while leaving some room for carefully limited work obligations, family responsibilities, or both.
- Standard outpatient care: This is lighter-touch treatment and is often better used for step-down care, maintenance, or continued accountability after stabilization.
The mistake many executives make is choosing outpatient because it appears less disruptive. Lower disruption only helps if the home environment is stable, the psychiatric picture is contained, and the client can follow through consistently without close supervision. If those conditions are missing, outpatient care can preserve the calendar while delaying real progress.
For professionals asking whether treatment can coexist with active responsibilities, some treatment options for people who can't completely stop working can be appropriate. The decision should be based on clinical fit, not wishful scheduling.
Practical rule: As medical risk, psychiatric instability, or environmental pressure increase, flexibility becomes less useful and structure becomes more protective.
The Inpatient Advantage Privacy Focus and Career Continuity
A managing partner is answering late-night messages, covering visible lapses with performance, and telling himself he can handle treatment around his calendar. In practice, that arrangement often protects the schedule more than the person. For high-achieving professionals with substance use, burnout, anxiety, depression, or trauma operating together, residential care can provide the first setting quiet enough for accurate assessment and fast course correction.

Why privacy improves clinical work
Privacy is not just a comfort issue. It affects what gets said, what gets observed, and how quickly treatment can work.
In residential care, clinicians see the full day instead of a narrow outpatient window. Sleep disruption, panic, irritability, medication side effects, cravings, compulsive work habits, and interpersonal patterns become visible in context. For clients with dual diagnosis needs, that matters because substance use and psychiatric symptoms rarely stay in separate lanes. The National Institute on Drug Abuse notes that inpatient and residential settings can be appropriate when a person needs a structured environment with around-the-clock support, especially when co-occurring conditions are part of the picture, in its overview of treatment approaches for drug addiction.
Disclosure also changes in a protected setting.
Senior professionals often filter themselves in outpatient care because they are still managing image, access to substances, family pressure, and a constant stream of decisions. Remove those pressures for a period of time, and the clinical team can address what is driving the pattern, not just the visible drinking, drug use, or emotional volatility.
Why inpatient can protect career continuity
Executives usually do not ask whether treatment matters. They ask whether treatment can be done without unnecessary professional damage.
Well-run executive programming answers that question with structure. Limited device access, scheduled work blocks, private accommodations, and clear boundaries around contact with the office can preserve key responsibilities without letting work retake the day. For some clients, that balance is the difference between postponing care and entering treatment early enough to prevent a larger personal or professional failure. Clients considering executive inpatient mental health treatment with clinically managed work access are usually weighing exactly that trade-off.
I often tell professionals the same thing. A short period of controlled absence is usually easier to contain than months of inconsistent judgment, strained relationships, and declining reliability that colleagues can already see.
The investment question
Residential care costs more upfront. That is true.
For the right client, the better calculation is broader than the admission fee. The true comparison is residential treatment versus another quarter of impaired decision-making, hidden symptoms, legal or regulatory exposure, preventable family fallout, and a worsening psychiatric picture that becomes harder to stabilize while work demands stay high.
Outpatient care can be appropriate for a stable professional with solid support at home and enough psychological bandwidth to follow treatment closely. Inpatient care earns its value when privacy, containment, and daily clinical oversight protect both recovery and the life the client is trying to preserve.
A Detailed Comparison for the Discerning Client
A senior executive can usually keep a strained quarter from public view. Treatment selection is harder to hide from consequences. The better question is which setting gives this person the highest chance of fully engaging, stabilizing, and returning with judgment, credibility, and follow-through intact.
For professionals, the decision is rarely about comfort. It is about fit. The right level of care depends on psychiatric complexity, work pressure, privacy needs, home stability, and whether prior attempts have already shown that partial treatment access is not enough.
| Factor | Luxury Inpatient (Residential) | Intensive Outpatient (IOP) |
|---|---|---|
| Clinical intensity for dual diagnosis | Better suited to clients who need daily observation, frequent medication review, immersive therapy, and separation from triggers | Better for clients who are stable enough to live at home and practice skills between sessions |
| Privacy and confidentiality | Greater control over environment, peer exposure, and outside contact | More exposure to workplace, family, and social visibility because daily routines continue |
| Career integration | Can work well when the program permits structured electronics access and protects treatment hours | Offers more scheduling flexibility, but work often spills into treatment time |
| Medical safety during detox | Better choice when withdrawal, medication complexity, or psychiatric instability may require close monitoring | Poor fit when early stabilization is uncertain or medically risky |
| Home and trigger exposure | Removes the client from alcohol, drugs, conflict, and conditioned routines | Requires the client to face the same environment that may be reinforcing use |
| Completion risk | Contained setting usually supports follow-through | Higher risk of missed sessions or early dropout when stress and logistics stay active |
Completion matters more than preference
Completion is not a minor metric. It is one of the clearest signals that the treatment setting matched the client's actual needs.
A national treatment episode analysis published by SAMHSA reported higher completion in residential treatment than in outpatient treatment, with residential care associated with greater odds of finishing treatment after adjustment for client and system factors, as summarized in this SAMHSA treatment episode analysis resource. For high-achieving professionals, that distinction matters because convenience often gets mistaken for suitability.
I see this often with executives who are accustomed to performing under pressure. They choose the setting that appears least disruptive, then discover that every unresolved demand still has direct access to them. Meetings expand. Travel resumes. Family obligations fill the remaining space. Treatment becomes one more item on an overcrowded calendar instead of the central intervention it needs to be.
The hidden trade-offs
Strong outpatient candidates usually have several conditions already in place.
- A stable home base: The residence is calm, substance-free, and not organized around drinking, drug use, or chronic conflict.
- Reliable follow-through: The client can attend consistently, report accurately, and act on recommendations without repeated drift.
- Lower immediate medical risk: Withdrawal concerns, suicidality, and major psychiatric destabilization are not driving the presentation.
- Support that helps rather than enables: A spouse, family member, assistant, or close friend can reinforce treatment boundaries instead of protecting the old pattern.
Residential care becomes the stronger strategic choice when those conditions are weak, absent, or actively working against recovery.
When residential is the stronger strategic call
Consider residential first when the client presents with any combination of the following:
- Dual diagnosis complexity: Substance use is entangled with anxiety, trauma, depression, insomnia, grief, burnout, or mood instability.
- Repeated failed attempts: The client has tried to cut back, change substances, rely on therapy alone, or complete outpatient treatment without durable progress.
- Concealment supported by success: Professional status has made the problem easier to hide, while the underlying clinical picture continues to worsen.
- High-consequence leadership: The person's decisions affect employees, investors, patients, clients, or family systems in ways that make impaired judgment unusually costly.
A polished presentation can obscure a high-acuity case. Titles, income, and public composure do not reliably indicate that outpatient care is enough.
When intensive outpatient can be appropriate
IOP can work well for a disciplined professional with lower destabilization, strong support, and a home environment that does not constantly reactivate the problem. It gives the client a chance to practice recovery skills in real time, under ordinary pressure, while staying connected to work and family life.
It also asks more of the client. Honesty has to be better. Boundaries have to hold. Treatment cannot remain negotiable every time a demanding week appears.
One factual example of an executive-focused residential option is Reflections, a California-licensed, Joint Commission-accredited provider for adults with co-occurring mental health and substance use disorders. Its model includes private rooms, clinically managed detox support, dual-diagnosis treatment, and appropriate access to electronics for clients who must maintain some professional contact.
Outcomes Relapse Risk and Long-Term Success
A partner returns from treatment clear-headed, motivated, and certain the problem is under control. Two weeks later, the calendar fills, sleep drops, travel resumes, and the old pressure cycle starts again. The question is no longer which setting looked stronger on admission. The question is whether the treatment plan was built to hold under real executive conditions.
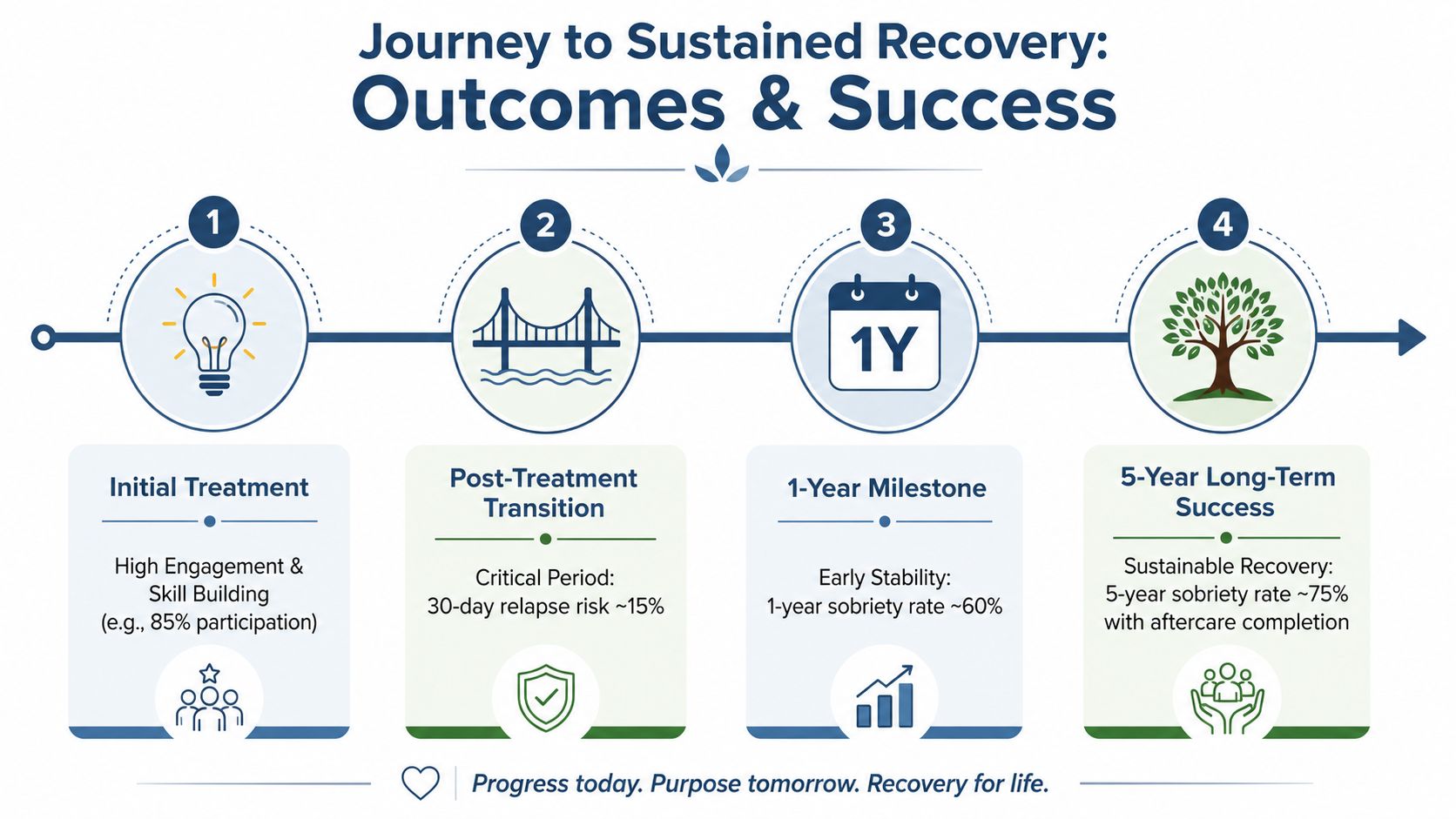
Why early gains need protection
Outcomes improve when care is treated as a sequence rather than a single event. Evidence reviews summarized by the National Center for Biotechnology Information have noted that residential care often produces stronger early stabilization, while long-term success depends heavily on continuing treatment after discharge.
That pattern is familiar in executive cases.
Residential treatment can create enough distance from substances, overwork, poor sleep, and constant demands to get an accurate clinical picture. It gives the team time to sort out what is driving the substance use. Anxiety, depression, trauma, burnout, bipolar symptoms, and sleep disruption often sit underneath the visible behavior. If those factors are missed, early improvement can look better than it is.
Outpatient care serves a different purpose. It tests recovery where it has to function. At home. In meetings. During conflict. On the road.
Where relapse risk rises for professionals
High-achieving clients rarely relapse because they lack intelligence or insight. More often, they relapse because success has trained them to override limits that recovery requires.
The usual pattern is predictable:
- A crisis forces treatment: A family rupture, performance concern, legal scare, or health issue finally interrupts denial.
- Early improvement creates false confidence: Sleep improves, substances stop, and the client assumes clarity means lasting stability.
- Work regains control: Therapy attendance slips, accountability weakens, and private stress returns faster than the treatment structure does.
For professionals, relapse is not only a return to use. It can show up first as irritability, secrecy, overwork, emotional withdrawal, risky prescribing patterns, or a sharp drop in judgment. By the time alcohol or drug use is visible again, the professional and family costs may already be substantial.
What long-term success usually requires
The stronger model uses each level of care for its actual job.
- Residential care: Stabilize the client, manage withdrawal risk when present, complete psychiatric and medical assessment, and begin serious dual-diagnosis treatment in a private setting.
- Outpatient care: Practice boundaries and coping skills under normal pressure while keeping close clinical contact.
- Continuing care: Maintain therapy, medication oversight when indicated, recovery accountability, and family or couples work long enough for change to become reliable.
In my experience, professionals do best when treatment protects both recovery and decision-making capacity. That means judging success by more than abstinence. The better questions are whether the client can tolerate stress without reaching for a substance, tell the truth sooner, repair trust at home, and return to leadership without the private instability that was already affecting performance.
For this population, the right level of care is a strategic choice. It reduces relapse risk, protects reputation, and gives recovery a structure strong enough to survive real life.
Real-World Scenarios Deciding What Fits Your Life
Abstract guidance helps. Real life decides.

Scenario one
A chief executive has been using alcohol nightly and prescription medication intermittently for sleep and anxiety. There's trauma history, worsening irritability, and growing emotional distance at home. The board doesn't know the full extent, but leadership judgment is slipping.
Residential care is usually the stronger choice. This client needs privacy, full psychiatric review, close monitoring during early stabilization, and enough time away from triggers to address the underlying drivers rather than just the visible behavior.
Scenario two
A senior manager has developed problematic drinking but still has a stable marriage, a supportive home, and no major withdrawal concerns. The substance use is serious, but the person remains motivated, accountable, and willing to organize work around treatment.
An intensive outpatient model may fit. It allows the person to keep practicing new boundaries in real time while still receiving structured therapeutic support several times each week.
Scenario three
A founder has already tried outpatient therapy and brief abstinence periods but keeps returning to stimulant use under stress. The company is entering a demanding phase, and the founder insists on remaining available for essential decisions.
This is often where executive-style inpatient care becomes especially useful. The client may need residential treatment first, with carefully bounded access to devices for limited business continuity, followed by step-down outpatient support once stability is established.
The deciding questions
The right fit usually becomes clearer when these questions are answered:
- What happens when stress spikes: Does the person use immediately, isolate, rage, panic, or become unreliable?
- What is home like: Supportive and calm, or tense, enabling, and full of cues tied to use?
- Has lower-intensity care already failed: If yes, repeating it for convenience rarely changes the outcome.
- Is work a reason for flexibility, or a reason treatment keeps getting diluted?
These answers matter more than title, income, or appearance.
Taking the Next Step Toward Executive Recovery
For professionals, choosing between inpatient and outpatient rehab isn't about optics. It's about matching the level of care to the level of risk. The right decision protects health, family life, and professional function at the same time.
The strongest next step is a confidential clinical assessment. That process should look at substance use severity, withdrawal risk, co-occurring mental health symptoms, home environment, work demands, and prior treatment history. It should also account for how much privacy, structure, and monitored support the client needs, not how much they would prefer to need.
When the clinical picture is complex, luxury residential care often provides the depth that outpatient treatment can't replicate at the start. When the client is stable enough to remain at home, outpatient work can be highly effective. For many executives, the most sensible path includes both. Residential first, then a structured step-down plan that protects the gains made in treatment.
A discreet program for this population should offer licensed clinical care, dual-diagnosis capability, private accommodations, thoughtful family involvement, and practical support for professional continuity where appropriate. Those details aren't cosmetic. They often determine whether a high-performing client engages fully or stays half in, half out.
Reflections provides confidential luxury dual-diagnosis treatment in California for adults who need residential care that respects both clinical complexity and professional life. Its setting includes private rooms, Joint Commission-accredited care, PhD-level clinicians, detox support, and appropriate access to electronics for clients who must remain selectively connected while doing serious treatment work.









