A senior executive closes the laptop after another late call, pours a drink, and tells themself it's temporary. The deal pressure will ease. The sleep will improve. The pills are just for focus. The alcohol is just to come down. Outwardly, nothing looks broken. Revenue is up, the calendar is full, and colleagues still describe that person as disciplined, high capacity, and reliable.
Privately, the experience is very different. There's fear of being found out, fear of losing authority, fear of becoming “the problem” in a life built around competence. For high-performing professionals, addiction rarely arrives as obvious collapse. It often hides inside achievement, routine, and image management. That's why shame and addiction become so tightly linked in this population. The substance use is painful. The threat to identity can feel even worse.
The Professional's Dilemma with Shame and Addiction
For professionals, shame doesn't just sound like regret. It sounds like, “If anyone knew, everything could unravel.” Career standing, licensure, leadership credibility, family reputation, and financial responsibility all become part of the emotional equation. The result is a form of suffering that's highly organized and extremely private.
Public health commentary recognizes that shame and stigma operate differently across populations, and for high-functioning adults and professionals, shame is often intensified by fear of professional and social fallout. It also notes that treatment environment and language matter, because less discreet settings can intensify shame and contribute to delayed help-seeking and dropout, as discussed in guidance on reducing the stigma of addiction at work.
Why success can make the problem harder to admit
High achievers usually know how to compensate. They can still present well in meetings, still answer emails at midnight, still outperform peers for a long stretch. That competence becomes a shield. It also becomes a trap.
A professional may interpret addiction through a performance lens rather than a clinical one:
- Missed boundaries become “commitment.” Working excessively can hide the fact that substances are being used to sustain output or blunt distress.
- Isolation looks productive. Skipping dinners, vacations, or personal conversations can be framed as focus when it is concealment.
- Control becomes the story. Many professionals delay treatment because they believe they should be able to solve the problem privately.
Shame in professionals often attaches to identity first and symptoms second. That's why telling someone to “just get help” often misses the point.
Why generic treatment often fails this audience
A successful professional usually isn't asking only, “How do I stop using?” They're also asking, “How do I do this without destroying everything I've built?” If a program ignores confidentiality, professional pressures, and the realities of public visibility, it can deepen the very shame that needs treatment.
That's the central clinical issue. Shame isn't just a byproduct of addiction. In many professionals, it becomes one of the forces that keeps addiction in place.
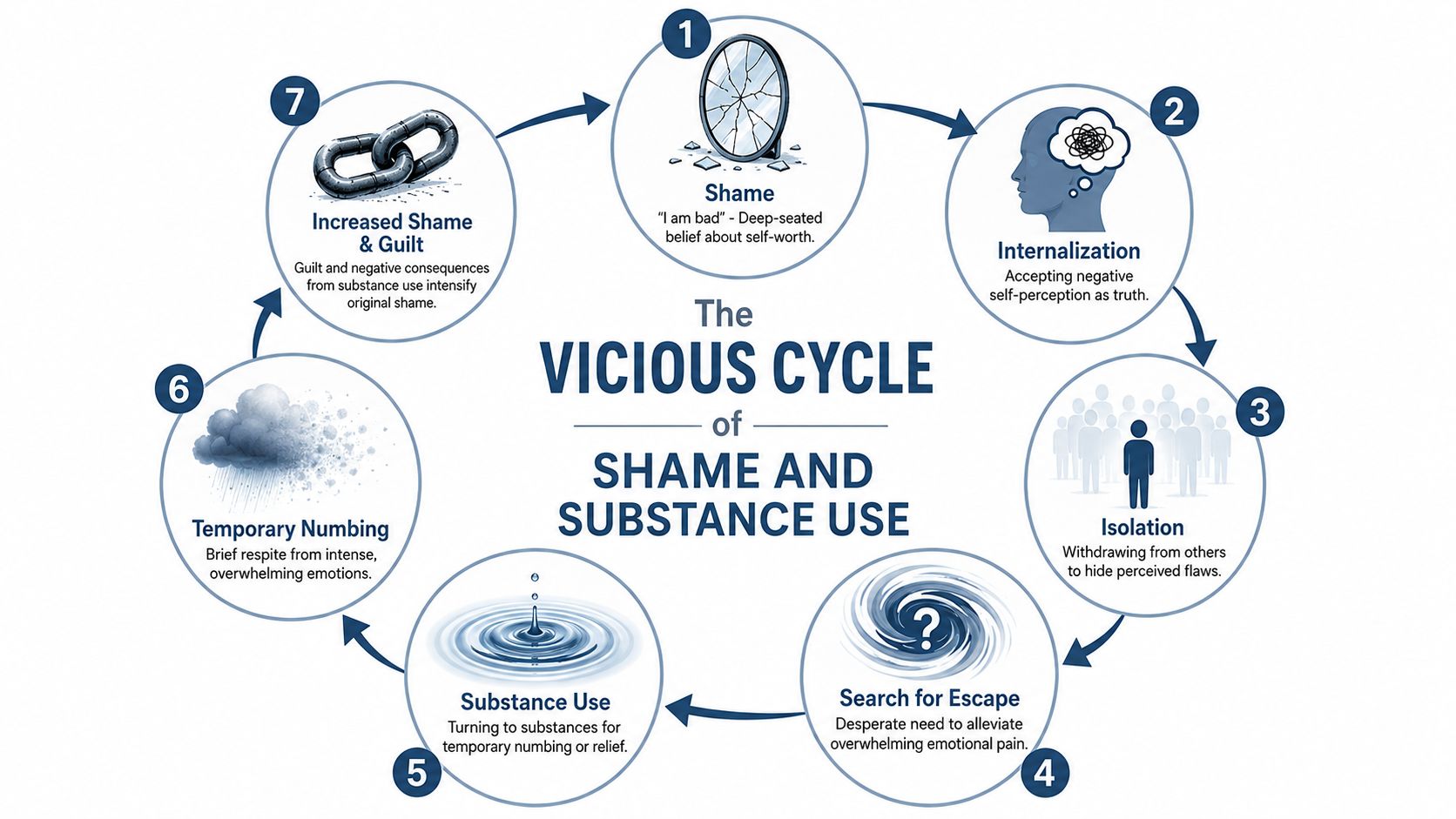
The Vicious Cycle of Shame and Substance Use
Guilt says, “I did something bad.”
Shame says, “I am bad.”
That distinction matters. Guilt can support repair. It can lead a person to apologize, change course, and reconnect with their values. Shame is more corrosive. It attacks identity, not behavior. When that happens, the mind stops looking for solutions and starts looking for escape.
Why shame pulls professionals deeper
For a high-functioning person, shame often grows in silence. A partner notices distance. A colleague comments on irritability. Sleep becomes irregular. Medication, alcohol, or other substances start serving a purpose. They reduce agitation, mute self-criticism, or help a person perform on demand. Relief appears quickly, but it doesn't last.
Then consequences follow. They may be subtle at first. More secrecy. More rationalization. More dependence on being “on.” Those consequences create fresh guilt and reinforce the original shame. The person doesn't just think they made a mistake. They start to feel completely compromised.
The cycle in plain terms
This is what the loop often looks like in practice:
- A painful self-judgment forms. The person feels inadequate, fraudulent, weak, or defective.
- They hide the struggle. Openness feels too risky, so they withdraw emotionally while maintaining appearances.
- Emotional pressure builds. Stress, exhaustion, and inner criticism intensify.
- A substance offers relief. It numbs, energizes, slows down, or distracts.
- The relief fades. The original problem is still there, often with new consequences attached.
- Shame grows. The person feels worse about who they are and less likely to ask for help.
- Use becomes easier to justify. The cycle restarts.
Clinical reality: Shame behaves like psychological quicksand. The harder someone tries to escape it alone through concealment and control, the deeper they sink.
This isn't just theory. In a longitudinal study of adults with stimulant use disorder, higher baseline shame predicted a slower decline in stimulant use over time, which suggests shame can function as a maintenance variable in recovery rather than merely a side effect of addiction, according to this longitudinal research on shame and stimulant use disorder.
For professionals, that finding has practical weight. If treatment focuses only on abstinence goals, symptom monitoring, or external accountability, but leaves shame untouched, the deeper engine of relapse may still be running.
How Shame Changes Your Brain
Shame isn't “just in someone's head” in the casual sense. It has a measurable neural footprint. That matters because many professionals interpret shame as weakness or lack of discipline, when it's closer to a whole-body threat response that drives hiding, freezing, and avoidance.

The shutdown pattern behind secrecy
A meta-analysis of 17 shame and embarrassment studies found activation in the left anterior insula, associated with emotional awareness and arousal, along with shame-specific recruitment of the dorsal anterior cingulate, thalamus, and premotor cortex. These regions are tied to social pain and behavioral inhibition, as described in this meta-analysis on the neural basis of shame.
In plain language, shame can push the brain toward a shutdown state. A person becomes highly aware of threat and highly inhibited about action. That combination is one reason shame so often produces concealment instead of reflection.
What this looks like in a working professional
A professional under shame pressure may still appear composed. Inside, the process is different:
- Social exposure feels dangerous. Honest disclosure to a spouse, physician, or colleague can feel biologically loaded, not merely uncomfortable.
- Decision-making narrows. Instead of asking, “What would help?” the mind asks, “How do I avoid being seen?”
- Behavior becomes defensive. The person cancels appointments, minimizes symptoms, or delays treatment even while recognizing the problem.
Shame often drives withdrawal before it drives insight. That's why waiting for someone to “hit bottom” is poor clinical strategy with high-functioning adults.
Because shame is linked to behavioral inhibition, many clinicians use body-based regulation alongside psychotherapy. Tools that support down-regulation can help a person stay engaged long enough to think clearly and tolerate vulnerability. For readers interested in practical nervous-system strategies, this overview of vagus nerve activation for recovery offers a useful starting point.
The key takeaway is simple. If shame pushes the brain toward hiding, treatment has to lower threat, protect dignity, and create enough safety for honest participation. Otherwise, intelligence and self-control get recruited into avoidance.
Recognizing Addiction in High-Functioning Professionals
The signs of addiction in executives and professionals rarely match the stereotype. There may be no public blowup, no obvious financial collapse, no dramatic disappearance from responsibility. In fact, many people in this position become more outwardly productive while their private life narrows and their internal strain intensifies.
That's why recognition depends less on visible chaos and more on pattern detection.
Signs that are easy to miss
A high-functioning professional may present with:
- Precision that has become rigid. Perfectionism can hide fear, overcompensation, and an increasing inability to tolerate mistakes.
- Work as camouflage. Long hours may reflect ambition, but they can also reduce scrutiny and create cover for isolation.
- Irritability mislabeled as stress. The person seems shorter, less flexible, and more reactive, especially when routines are interrupted.
- Selective withdrawal. They remain fully available for business obligations but pull back from family, friendships, and restorative activities.
- Substance use with a job description. Alcohol for networking, stimulants for output, sedatives for sleep, or prescription misuse for “performance” all get framed as necessary tools.
Many professionals also become highly skilled at presenting partial truths. They'll disclose insomnia but not the medication pattern. They'll mention burnout but omit the drinking. They'll seek help for anxiety while trying to keep the substance issue outside the conversation.
What a proper assessment should include
A nuanced evaluation has to look beyond the substance itself. It should ask what role the substance is playing and what emotional state it's protecting the person from. In professionals, that often means examining trauma history, mood symptoms, anxiety, sleep disruption, perfectionism, and self-stigma.
A thorough assessment should clarify:
- Whether there's a co-occurring mental health condition such as depression, anxiety, trauma-related symptoms, or another driver of self-medication
- How shame shows up behaviorally, including concealment, avoidance, and dropout risk
- What professional realities matter, including licensure concerns, family exposure, public visibility, and work demands
Readers who want a more detailed picture can review hidden signs of addiction in executives, especially if the concern is that things still look “functional” from the outside.
The best assessments don't ask whether someone has failed enough to deserve help. They ask what's being managed, what's being hidden, and what conditions will let the person tell the truth safely.
Evidence-Based Therapies to Heal Shame
A senior executive can discuss market risk, litigation exposure, and headcount decisions with total composure, then shut down the moment therapy touches the words "I felt ashamed." That reaction is common in high-performing professionals. Shame is rarely a lack of insight. It is a threat response tied to identity, status, and fear of professional ruin.
Treatment has to match that reality. Approaches built around pressure or public confession often increase concealment in people whose careers depend on control, precision, and credibility. Effective care reduces secrecy without stripping away dignity.
What often undermines progress
Shame-linked addiction tends to worsen under treatment models that miss the function shame serves.
- Advice alone does not change behavior. High-achieving adults usually know what they should do. The gap is not information. It is the inability to tolerate the emotional fallout that follows honesty, rest, or imperfection.
- Confrontation can increase hiding. If a professional already expects judgment, a harsh approach confirms the belief that exposure is dangerous.
- Substance-focused care can stay too shallow. Abstinence matters, but recovery is less stable when treatment never addresses the self-attack, fear, and avoidance driving the use.
A useful clinical standard is simple. Hold people accountable in a way that preserves self-respect.
Therapies that treat the mechanism of shame
No single therapy covers every part of shame. In practice, the strongest treatment plans combine methods that address distorted beliefs, nervous-system activation, avoidance, and old relational injuries.
| Therapy | How it helps heal shame |
|---|---|
| CBT | Identifies rigid beliefs such as "If I need help, I am failing" and replaces them with more accurate thinking. |
| DBT | Builds distress tolerance and emotion regulation so shame does not immediately trigger drinking, drug use, or shutdown. |
| ACT | Helps people act from values rather than from self-criticism, fear, or perfectionism. |
| Motivational Interviewing | Lowers defensiveness and strengthens honest engagement, especially in professionals who feel cornered by treatment. |
| Trauma-informed therapy | Examines whether chronic shame began as an adaptation to earlier humiliation, criticism, neglect, or instability. |
| Somatic and experiential therapies | Addresses the bodily side of shame when insight is present but the nervous system still reacts as if exposure is dangerous. |
Why these approaches work for high-functioning professionals
CBT is often a strong starting point because professional shame usually has a performance logic. Patients say things like, "Competent people do not fall apart," or, "One mistake cancels out years of success." Those beliefs can be examined, tested, and revised in treatment. A structured CBT approach within dual-diagnosis treatment is particularly useful when substance use and self-criticism reinforce each other.
DBT helps when the problem is speed. Many executives can explain their behavior clearly after the fact, but that insight disappears once stress spikes. A difficult board call, a licensing concern, a conflict at home, or a threat to reputation can trigger shame fast. DBT gives practical skills for getting through that window without reaching for alcohol, sedatives, stimulants, or compulsive work.
ACT is valuable because it changes the person's relationship to the inner voice. The goal is not to win an argument with every harsh thought. The goal is to notice the thought, reduce its control, and choose behavior that fits the person's values. For readers working on taming your inner critic, that shift is often a turning point.
Trauma work often changes the prognosis
In many professionals, shame did not start with the addiction. It started much earlier, in environments where approval depended on achievement, mistakes brought humiliation, or vulnerability was treated as weakness. Substance use then became a fast way to quiet the alarm.
That history changes treatment planning. Therapy has to address current behavior and the older learning that taught the person to hide, overperform, or numb out. At Reflections, that can include psychiatric care, individual psychotherapy, skills work, and adjunctive therapies in a private residential setting for adults with substance use and co-occurring anxiety, trauma, depression, or related conditions.
Shame is not only cognitive
Professionals often stay in analysis because analysis feels safer than emotion. They can describe the pattern in detail and still remain trapped inside it.
This is why nonverbal methods matter. Somatic work, mindfulness, and experiential therapies help patients notice what happens in the body before relapse. Tightness in the chest, a collapse in posture, a surge of heat, the urge to disappear, the need to regain control. Once those signals are recognized early, they can be treated early.
Recovery becomes more durable when thinking, physiology, and behavior change together.
Balancing Recovery with Your Career
The most common reason professionals postpone treatment isn't lack of intelligence. It's fear of fallout. They assume recovery requires disappearing from work, losing control of communication, or creating a chain reaction of questions they aren't ready to answer. For many executives and high earners, those concerns are serious and legitimate.
A treatment model that ignores career reality can increase resistance before therapy even starts.

Why flexibility matters clinically
For some professionals, access to electronics isn't a luxury feature. It's part of what allows treatment to happen at all. Being able to retain a phone or laptop, when clinically appropriate, can reduce panic, preserve essential responsibilities, and make it possible to practice new coping skills in real time rather than in a vacuum.
That benefit is often misunderstood. The goal isn't uninterrupted productivity. The goal is supported exposure to reality. A person receives a difficult email, notices the stress response, and works through it with clinical support instead of defaulting to substance use.
Privacy changes participation
Private rooms matter for the same reason. High-level professionals often need confidential space for sensitive conversations, focused work blocks, or decompression after demanding sessions. Beyond these practical needs, privacy reduces performative coping. A person can stop managing the room and start engaging the treatment.
This is often where shame begins to loosen. Not because pressure disappears, but because treatment no longer feels like another threat to identity.
A few practical criteria help professionals evaluate fit:
- Does the setting protect confidentiality in a meaningful way? Privacy has to be operational, not just promised.
- Can the client stay connected to urgent responsibilities when appropriate? That flexibility lowers the barrier to entry.
- Is the environment calm enough to support deep work? High stimulation and poor discretion can amplify shame.
Recovery works better when treatment respects the life the person is trying to preserve, while also confronting the patterns that life has been organized around.
Many professionals also need help with the internal pressure that follows them everywhere. For a practical look at reducing self-attack between sessions, this article on taming your inner critic can complement clinical work.
Recovery doesn't require abandoning ambition. It requires rebuilding the way ambition is carried, so performance no longer depends on secrecy, exhaustion, and chemical relief.
Your Confidential Path to Recovery
Shame and addiction feed each other in ways that are especially punishing for successful professionals. The person looks capable, so other people miss the severity. The person is capable, so they keep trying to manage it alone. That combination can delay help far longer than it should.
A more useful path is usually simpler than people expect.
Three decisions that change the trajectory
- Acknowledge the problem without turning it into an identity statement. The issue is that there's a struggle requiring treatment, not proof of personal failure.
- Get a confidential assessment that looks at the full picture. Substance use, mental health, stress load, sleep, trauma history, and shame patterns all matter.
- Choose a setting that matches the reality of professional life. Privacy, clinical depth, and appropriate flexibility often determine whether someone stays engaged.
Some people wait until consequences become public because they think that's when treatment becomes justified. That's backward. Earlier intervention is often what protects career, family, and health.
The opposite of shame isn't self-excuse. It's honest, supported responsibility.
For high-functioning adults, the right treatment environment doesn't minimize accountability. It makes accountability possible by reducing threat, protecting dignity, and addressing the emotional system that has kept the addiction in place.
A confidential conversation with Reflections can help clarify whether a private, professionally compatible treatment setting is the right next step. For executives, business owners, and other high-achieving adults, the goal isn't to choose between recovery and career. It's to begin treatment in a way that protects privacy, addresses shame directly, and supports lasting change.









