The most common advice on OCD and substance abuse gets one thing dangerously wrong. It assumes the rule-bound, perfectionistic nature of OCD protects people from addiction. In practice, that belief causes families, physicians, and even highly capable professionals to miss the problem until it has already become entrenched.
That mistake is even more costly in executive and high-performing populations. A person can still run meetings, protect a reputation, answer late-night emails, and close deals while privately relying on alcohol, sedatives, or other substances to quiet intrusive thoughts, blunt anxiety, or make compulsive routines feel manageable. From the outside, it can look like stress. Clinically, it often looks like a dual diagnosis that needs complex, integrated care.
The Unexpected Link Between OCD and Addiction
The old protective theory doesn't hold up. A large Swedish cohort study involving over 6.3 million individuals found that OCD was associated with a 3.7-fold increased risk for any substance misuse outcome and a 6.7-fold higher risk for drug-related disorders, directly challenging the idea that OCD somehow shields people from addiction, as discussed in this analysis of co-occurring disorders and supported by the 2023 Swedish cohort findings summarized here.
For executives and other high-achieving professionals, that finding matters because OCD often hides behind traits that workplaces reward. Precision. Control. Intensity. Relentless standards. Those qualities can camouflage real psychiatric distress for a long time.
Why high performers are often missed
A professional with OCD may not look disorganized or impaired. The person may look unusually disciplined. That's part of the problem.
Common patterns include:
- Rigid excellence that earns praise: Rechecking, overpreparing, and perfectionism can be mistaken for leadership standards.
- Private distress behind public competence: Intrusive thoughts and compulsive rituals often stay hidden because the individual fears shame, exposure, or loss of status.
- Substance use folded into success culture: A nightly drink to “decompress,” a sedative to force sleep, or a substance used to mute mental noise can seem functional until dependence develops.
Standard patient education often misses the contradiction. OCD may look controlled from the outside while addiction risk is rising underneath.
Families often say the same thing in different words. They assumed the person was too disciplined to develop a substance problem. In reality, the very effort required to manage untreated OCD can create relentless internal pressure, and substances can become a fast, private form of relief.
What this means clinically
OCD and substance abuse shouldn't be treated as two separate problems that happen to exist at the same time. In many cases, they operate as a connected system. The obsessive fear drives distress. The distress drives substance use. The substance use then makes the psychiatric picture harder to stabilize.
That's why generic advice falls short. High-functioning clients need careful assessment that looks beyond surface performance and identifies what's maintaining the cycle.
The Vicious Cycle of Self-Medication
For many people, OCD and substance abuse begins with relief-seeking, not recklessness. The person isn't trying to create a second disorder. The person is trying to get through the day with less terror, less mental noise, and less time trapped in compulsions.
A useful clinical analogy is fighting fire with gasoline. The substance may briefly suppress the immediate heat. Then it fuels the larger burn.
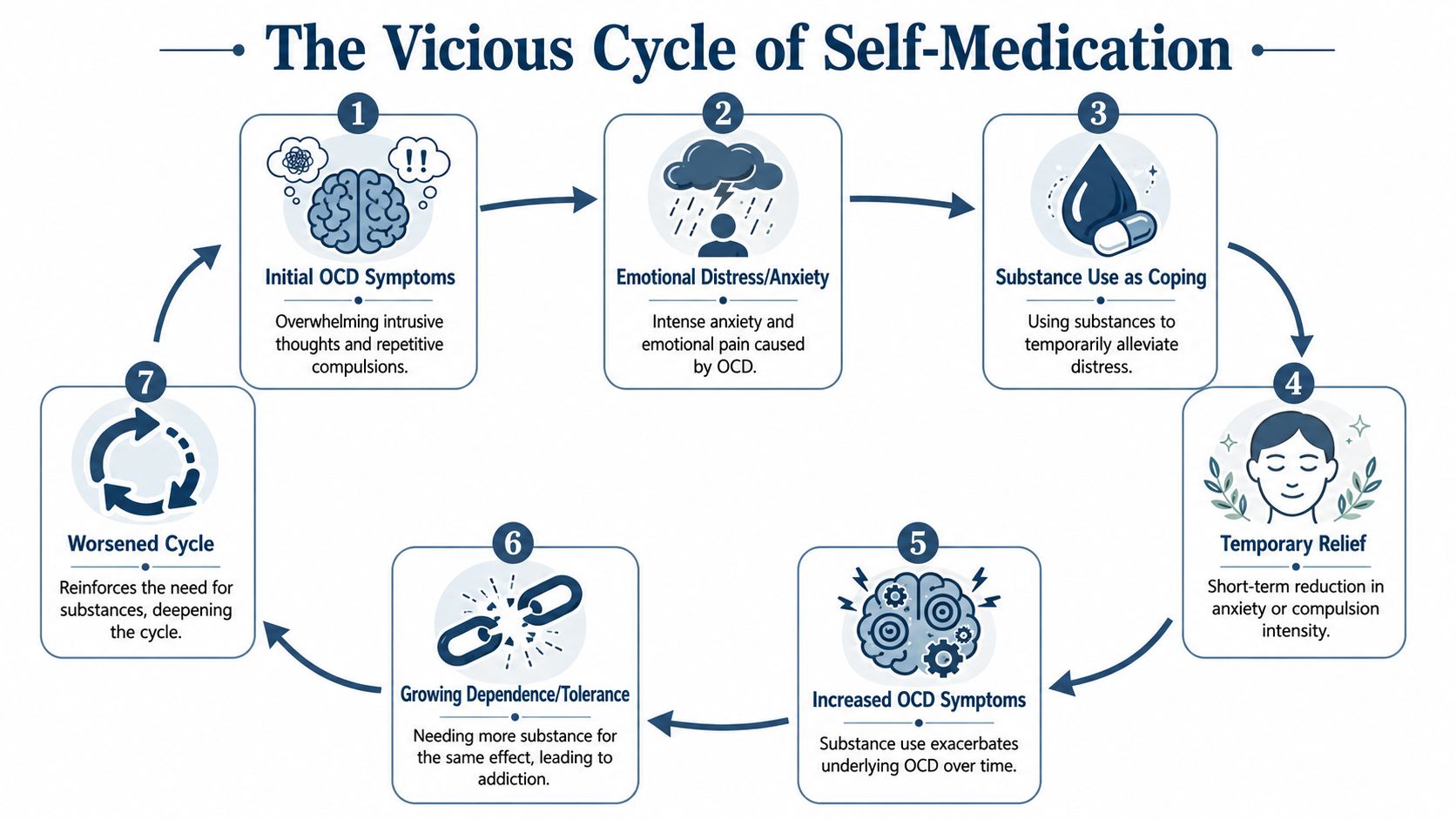
How the loop usually forms
The sequence is often straightforward:
- Obsessions create intense distress. Intrusive thoughts, doubt, contamination fears, moral fears, or checking urges drive sustained anxiety.
- Compulsions stop working well enough. The rituals may take more time, become less effective, or interfere with work and relationships.
- A substance offers quick relief. Alcohol may soften anxiety for a few hours. Sedatives may reduce agitation. Other drugs may blunt mental intensity or create escape.
- The brain learns the shortcut. Relief gets associated with the substance instead of with healthy coping or treatment.
- Symptoms rebound. Anxiety returns, often stronger, and OCD becomes less manageable.
- Tolerance and dependence build. More of the substance may be needed to produce the same effect.
- Both disorders tighten. The person now has worsening OCD and a substance problem.
Why sedatives are especially risky
The clinical significance of the data highlights that individuals with OCD have a 4.5-fold higher risk for alcohol-related disorders, a 6.7-fold higher risk for any drug-related disorder, and a 10.5-fold increased risk for sedative-related disorders compared to the general population, according to the JAMA Network Open cohort study.
That sedative finding is especially relevant in executive populations. High-responsibility professionals often don't present as chaotic users. They may present as exhausted, tightly wound, and unable to shut off. A sedative can look like a solution for sleep, tension, or anticipatory anxiety. Clinically, it can become the fastest route into a dangerous reinforcement loop.
Practical rule: If a substance is being used to “turn off” obsessions, reduce ritual-related anxiety, or force rest after mental overactivation, the treatment plan has to address OCD directly. Removing the substance without treating the driver usually won't hold.
What doesn't work
Several responses tend to fail:
- Willpower-only strategies: These ignore the underlying anxiety system.
- Performance-based denial: “Work is still getting done” isn't a psychiatric assessment.
- Treating the substance as the whole problem: That approach often misses why the person keeps returning to it.
The goal isn't just abstinence. The goal is to reduce the need for chemical relief by treating the obsessive-compulsive engine underneath it.
Recognizing the Signs in High-Functioning Professionals
In high-performing adults, OCD and substance abuse rarely announces itself in obvious ways. It tends to hide inside productivity, routine, and image management. Families often notice strain before they notice dysfunction.
A useful companion read on this pattern appears in hidden signs of addiction in executives, because executive impairment often looks very different from the public stereotype of addiction.
Behavioral signs at home and at work
The most revealing signs are often subtle:
- Secretive rituals around routine: Excessive checking, repeated reassurance-seeking, rigid scheduling, or unusual insistence on controlling environments.
- Substance use tied to transitions: Drinking after high-stakes meetings, relying on pills before flights, presentations, or sleep, or using substances to recover after obsessive overcontrol.
- Isolation disguised as workload: Canceling social plans, staying behind closed doors, and using “busy” as cover for compulsions or substance use.
Emotional indicators families often miss
OCD-related distress isn't always visible as panic. In professionals, it often shows up as irritation, shame, or emotional narrowing.
Watch for patterns such as:
- Sharp distress when routines are disrupted
- Disproportionate guilt or fear after small mistakes
- Increased defensiveness when asked about alcohol, medications, or sleep
- Mental exhaustion that doesn't improve with rest
A polished exterior can coexist with severe internal torment. Competence doesn't rule out a dual diagnosis.
Professional impact that gets rationalized
Many executives remain employed and externally successful deep into illness. That doesn't mean the problem is mild. It usually means the person has an unusually high capacity to compensate.
Professional warning signs include:
| Domain | What it can look like |
|---|---|
| Decision-making | Overchecking, delay, indecision, or needing excessive certainty before acting |
| Communication | Repeatedly revising messages, late-night emailing, or overcontrolling details |
| Leadership | Delegation problems, rigidity, and escalating distress when others don't follow exact processes |
| Recovery time | Needing substances to “come down” after ordinary work demands |
When loved ones see these patterns together, especially when anxiety, rituals, and substance use appear linked, the right next step isn't a confrontation built around blame. It's a confidential clinical evaluation that can distinguish stress, burnout, OCD, and addiction from one another.
Why Standard Addiction Treatment Often Fails for OCD
A substance-focused program often looks adequate on paper and falls apart in practice. The problem isn't effort. The problem is clinical mismatch.
A major review found that OCD onset precedes substance use in 70% of comorbid cases, with a median gap of 8 years, and that patients with both disorders often require 2 to 3 years longer treatment durations plus specific dual-intervention protocols that standard short-stay addiction programs don't provide, according to this systematic review of OCD and substance use comorbidity.
The core treatment error
If OCD is the earlier and often driving disorder, then addiction-only care treats the smoke while leaving the fire active. The client may detox successfully, complete groups, and understand relapse concepts. Then the untreated obsessions, compulsions, and anxiety surge back, and the old pressure for relief returns.
That's why standard substance education isn't enough for this population. A person can understand the consequences of relapse and still feel overrun by untreated obsessive fear.
What short-stay, one-size-fits-all care misses
Typical failure points include:
- No OCD-specific assessment: The program identifies anxiety broadly but doesn't map obsessions, compulsions, avoidance, and triggers.
- No exposure-based work: The client is told to reduce stress, even though OCD often requires structured therapeutic exposure rather than reassurance and avoidance.
- No integrated medication oversight: Psychiatric treatment may focus on detox comfort without addressing the full dual-diagnosis picture.
- No realistic time horizon: Executive clients with entrenched patterns often need a plan that matches the complexity of both disorders.
Treating addiction without addressing OCD often leaves the client sober but still trapped in the symptoms that drove substance use in the first place.
Why this matters for executives
A high-functioning professional can complete the wrong program and return to work looking improved while remaining clinically vulnerable. That scenario is common because achievement can mask incomplete stabilization.
For families, the key question isn't whether a program offers addiction treatment. Most do. The important question is whether the clinical team can treat obsessive-compulsive pathology and substance dependence at the same time, with enough depth to reduce relapse risk once the person re-enters a demanding environment.
The Gold Standard Integrated Treatment for Dual Diagnosis
When OCD and substance abuse occur together, parallel treatment isn't enough. The care has to be integrated. That means one coordinated plan, one shared clinical formulation, and one team treating both conditions as interdependent.
Research from the International OCD Foundation notes that treating both OCD and SUD simultaneously yields superior outcomes, including reduced OCD severity, longer treatment engagement, and higher abstinence rates at 12-month follow-up compared with treatment as usual, as described in this expert review on co-occurring OCD and substance use disorder.
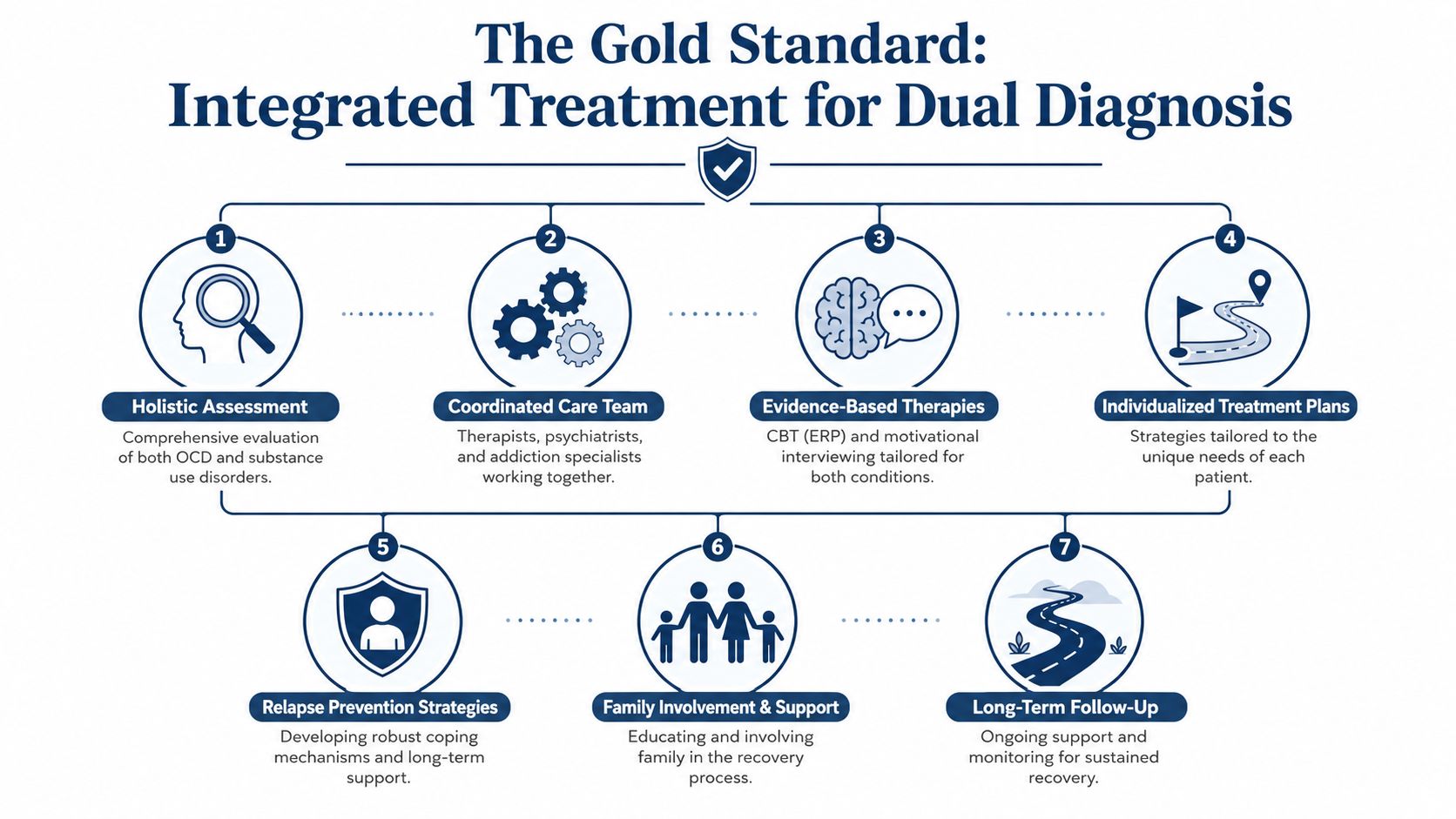
What integrated care actually includes
A strong program doesn't just alternate between addiction groups and mental health sessions. It combines methods in a way that makes clinical sense.
Essential elements include:
- A precise diagnostic assessment: The team needs to identify obsessions, compulsions, avoidance patterns, substance function, withdrawal risk, and co-occurring mood or trauma features.
- ERP within a broader therapy plan: Exposure and Response Prevention is central for OCD, but it works best when coordinated with addiction treatment, motivational work, and relapse planning.
- Psychiatric oversight with restraint and precision: Medication decisions should support stabilization without creating new dependency risks.
- Family education: Loved ones often unintentionally reinforce OCD through reassurance or reinforce addiction through crisis management.
How the therapies work together
Many families know the term CBT but not how it applies here. A clear overview of cognitive behavioral therapy helps explain the foundation. In dual-diagnosis care, CBT principles can support both OCD symptom work and substance-related thinking patterns, while ERP targets compulsions directly and DBT-informed skills help clients tolerate distress without using.
That combination matters because these clients don't just need insight. They need practice:
- sitting with uncertainty without ritualizing
- surviving distress without reaching for a substance
- identifying the specific moments when obsession turns into urge
- rebuilding routines that aren't organized around avoidance
One example of this model is integrated mental health and addiction treatment, where psychiatric care, psychotherapy, and addiction treatment are organized around the same case formulation instead of operating in silos.
The right treatment plan doesn't ask whether OCD or addiction is the “real” problem. It treats the pattern connecting them.
What tends to work best
Integrated treatment is most effective when the team is multidisciplinary and aligned. Psychiatrists, therapists, addiction clinicians, and family staff need to share the same goals and respond consistently. Mixed messages can quickly destabilize a client with obsessive doubt, high shame, and a strong drive to control uncertainty.
For executives, that sophistication isn't a luxury in the casual sense. It's often the difference between symptom management and real recovery.
Executive Care Redefined When to Choose Residential Treatment
For a high-level professional, the question usually isn't whether treatment is needed. It's whether treatment can happen without destroying privacy, continuity, and hard-earned credibility. That's why residential care for executives has to be designed differently from standard inpatient models.
One practical distinction is operational flexibility. Executive-focused residential programs may allow residents to retain personal electronics, including cell phones and laptops, so they can stay engaged with limited career obligations while receiving care, as outlined in this executive rehab overview.
When outpatient care usually isn't enough
Residential treatment becomes the strategic option when any of these conditions are present:
- Symptoms control the schedule: The person is organizing the day around rituals, recovery from substance use, secrecy, or both.
- Work pressure keeps sabotaging treatment: Every crisis, deadline, or leadership demand becomes a reason to postpone care.
- The home environment no longer supports stabilization: Privacy is gone, family tension is high, or substances remain too accessible.
- The person needs confidential, intensive assessment: High-functioning clients often need a period of separation from work intensity to see the pattern clearly.
Why the residential setting matters for this clientele
A luxury executive program isn't about image. It addresses real treatment variables that affect retention and honesty.
For working professionals, the most relevant features often include:
- Private rooms in detox and residential care: Privacy lowers exposure anxiety, supports sleep, and protects confidentiality.
- A clinically expert team: Dual-diagnosis clients need nuanced psychiatric and psychological treatment, not a generic addiction track.
- Structured access to electronics: The goal isn't to run the company from treatment. It's to preserve bounded, appropriate business continuity so treatment remains viable.
- An upscale, discreet environment: High-profile and high-earning individuals are more likely to engage fully when the setting matches the seriousness of the decision.
Executive dual-diagnosis treatment vs standard rehab
| Feature | Standard Rehab Program | Executive Residential Program |
|---|---|---|
| Work access | Often limited or prohibited | Structured access to phones and laptops when clinically appropriate |
| Accommodations | Shared or mixed privacy levels | Private rooms in detox and rehab |
| Clinical focus | Substance-first model | Integrated dual-diagnosis care for OCD and substance abuse |
| Pace | Uniform schedule for all clients | Individualized planning around symptom profile and professional realities |
| Privacy | Basic | Higher discretion for executives, public figures, and families |
| Treatment fit | General population approach | Designed for C-suite leaders, professionals, and high-responsibility clients |
Residential treatment is often the fastest way to protect both health and career when the current routine is quietly collapsing under the weight of untreated symptoms.
For many families, the turning point comes when they stop viewing residential care as an interruption and start viewing it as containment. It creates the protected space needed to stabilize the person before reputation, relationships, and health deteriorate further.
Sustaining Recovery and Preventing Relapse
Successful treatment isn't measured by discharge alone. OCD and substance abuse both have relapse potential, and high-achieving clients often return to environments filled with triggers such as pressure, overwork, sleep disruption, and the temptation to hide distress behind performance.
Long-term protection depends on a recovery plan that stays specific. Generic advice like “manage stress better” usually isn't enough. The plan should identify obsessional triggers, rituals, high-risk emotional states, and the exact moments when the urge to use substances tends to appear.
What protects recovery over time
Three areas matter most:
- Ongoing therapy with dual-diagnosis focus: The client needs continued work on OCD symptoms and substance-related coping, not one or the other.
- Relapse planning tied to executive life: Travel, public exposure, late work hours, decision fatigue, and isolation should all be addressed directly.
- Family participation: Loved ones do better when they understand reassurance traps, enabling patterns, and how to respond without escalating shame.
The long-term mindset
Recovery becomes more durable when the client stops aiming to look fine and starts learning how to live authentically, with structure, treatment compliance, and early intervention when symptoms spike. For professionals, this often includes rebuilding boundaries around work, sleep, stimulation, and secrecy.
The good news is that this dual diagnosis is treatable. With integrated care, a sophisticated aftercare plan, and the right level of discretion and support, people can return to demanding lives with more stability, clearer thinking, and far less dependence on compulsions or substances.
Reflections offers luxury dual-diagnosis treatment in a private residential setting for adults dealing with co-occurring mental health and substance use disorders, including OCD and substance abuse. For executives, C-suite leaders, and families seeking confidential care with private rooms, clinically managed detox, integrated psychiatric treatment, and appropriate access to electronics during treatment, it can be a practical next step to request a confidential assessment.









