The calendar is full. The phone never stops. Performance still looks intact from the outside, but the private reality has changed. Sleep is thinner, irritability is sharper, alcohol has shifted from social to functional, or a prescription that once seemed useful now feels necessary just to keep pace.
For many executives and high-performing professionals, the crisis doesn't arrive as public collapse. It arrives as quiet narrowing. Work remains excellent, but life outside work gets smaller, relationships become more strained, and internal distress gets managed with something that promises fast relief. Anxiety, depression, trauma, burnout, or mood instability often sit underneath that pattern. Substance use then becomes less of a party issue and more of a pressure-management system.
That combination has a name. It's often dual diagnosis, also called co-occurring disorders. And when that's the clinical picture, standard addiction treatment or stand-alone therapy usually isn't enough. Effective mental health and substance abuse treatment for this population has to be integrated, discreet, and structured in a way that protects both recovery and professional continuity.
The High-Achiever's Paradox
A senior professional can run a board meeting, negotiate a deal, and still be in real psychiatric and substance-related distress. High functioning isn't the same as healthy functioning. It often means someone has developed complex ways to conceal impairment, compensate for it, and keep producing long after the underlying system is under strain.

One common pattern looks like this: a leader begins using alcohol at night to shut off a racing mind. Over time, the drinking increases because the anxiety hasn't been treated. Sleep quality drops. Morning focus weakens. A stimulant, more caffeine, or another substance enters the picture to regain edge and composure. Outwardly, the person still appears competent. Internally, the system is becoming more brittle.
That's why the old stereotype of addiction misses the mark for this audience. Successful people often postpone care because they haven't lost everything. They're still earning, still operating, still convincing themselves that the issue is manageable.
Clinical reality: A person can be highly productive and still need intensive treatment.
That belief in self-management is common. In 2024, 48.4 million Americans aged 12 or older battled a substance use disorder, and among adults who needed treatment, a primary reason for not seeking it was the belief they could handle it on their own, 75.5% according to the Addiction Policy Forum summary of NSDUH findings.
Why professionals often miss the real diagnosis
Executives are trained to solve problems through discipline, intelligence, and endurance. That mindset helps careers. It can hurt recovery.
A few signs often point to a co-occurring picture rather than a simple “stress problem”:
- Relief-based use: Alcohol, sedatives, stimulants, or cannabis are being used less for enjoyment and more for sleep, focus, calm, or emotional escape.
- Escalating consequences at home: Work performance may still look acceptable, but a spouse, partner, or close family member sees irritability, withdrawal, secrecy, or volatility.
- Therapy that only half works: Insight improves, but symptoms and substance use keep cycling because both conditions aren't being treated together.
When a high achiever says, “Nothing is falling apart, but something is wrong,” that statement deserves clinical respect. It often signals the period when treatment can be most effective, before public damage, legal risk, or medical crisis force the decision.
Understanding the Dual Diagnosis Framework
Treating co-occurring disorders separately is like trying to kill one of two intertwined roots under the same tree. One root is mental health. The other is substance use. If treatment focuses on only one, the untreated root continues feeding the problem.

An executive with untreated panic symptoms may drink to slow the body down. Someone with depression may rely on stimulants to push through meetings and travel. A professional with trauma may use substances to blunt intrusive memories or emotional intensity. If treatment addresses the drinking or drug use without treating the panic, depression, or trauma, the person is left with the same internal drivers that made substance use feel necessary in the first place.
What integrated care actually means
Integrated care doesn't mean doing addiction work in one building and mental health work in another. It means one coordinated clinical plan addresses both conditions at the same time.
The World Health Organization and CDC both emphasize that co-occurring disorders should be treated through integrated care, combining medication and behavioral health rather than as separate conditions, as noted in the WHO guidance on mental health and integrated services.
In practice, that model usually includes:
- One diagnostic formulation: The team identifies how mood, anxiety, trauma history, sleep disruption, and substance use interact.
- One treatment plan: Therapy goals, medication decisions, relapse prevention, and functional goals are aligned instead of split apart.
- One clinical team conversation: Psychiatric, medical, and therapeutic staff work from the same map.
Separate treatment tracks often create separate stories. Recovery gets stronger when the team is treating one person, not two disconnected diagnoses.
Why this matters for analytical professionals
High-performing clients usually want more than reassurance. They want a coherent explanation for why they've kept repeating a pattern they can clearly see but haven't been able to stop. Dual diagnosis treatment provides that explanation.
For example, a professional with attention issues may have spent years self-medicating concentration problems, impulsivity, or restlessness. That's one reason resources on ADHD substance abuse can be useful for understanding how neurodevelopmental symptoms and addiction risk can intersect. The point isn't self-diagnosis. It's recognizing that substance use often has a functional role inside a larger psychiatric picture.
What doesn't work
Many professionals try one of three partial solutions.
| Approach | Why it falls short |
|---|---|
| Stopping substances without psychiatric care | The original anxiety, depression, trauma, or mood instability remains active |
| Treating only mental health | Substance use keeps disrupting mood, sleep, judgment, and therapy progress |
| Attending care that isn't integrated | Mixed messages and fragmented planning slow recovery |
A stronger option is a program built specifically around integrated dual-diagnosis treatment, such as integrated mental health and addiction treatment, where psychiatric care, therapy, and addiction treatment are designed to work in concert.
Inside a Clinically Sophisticated Treatment Program
A specialized program doesn't treat executives as if they need a motivational speech. It treats them as complex adults with layered symptoms, entrenched coping patterns, and legitimate performance pressures. The work is specific, clinical, and practical.
A thorough review found that evidence-based interventions like CBT have shown moderate significant effects versus minimal treatment, with a strong impact on reducing substance use frequency and quantity at early follow-up, according to the review in the National Library of Medicine database. That matters because high-functioning professionals often respond well when treatment is structured, intellectually honest, and directly tied to real-world behavior.
The core therapies and how they're used
CBT is often central because it helps identify the thought patterns that keep both symptoms and substance use in motion. For an executive, that may include perfectionism, catastrophic forecasting, black-and-white thinking, overcontrol, or the belief that rest is weakness. CBT makes those patterns visible and testable.
DBT becomes useful when the issue isn't only distorted thinking, but emotional intensity. Clients who swing between control and collapse, or who use substances after conflict, shame, or pressure spikes, often need stronger distress-tolerance and emotion-regulation skills.
ACT is especially relevant for professionals whose identity is fused with performance. It helps clients stop organizing life around avoiding discomfort and start acting from values, even when anxiety, grief, or uncertainty are present.
A serious program also uses motivational interviewing, not as a soft prelude, but as a disciplined method for working through ambivalence. Many executives do want help and still fear what treatment could mean for reputation, authority, or momentum. That conflict has to be addressed directly.
Medication is a precision tool
Medication management in dual diagnosis treatment should be careful, not casual. The goal isn't to medicate every feeling. The goal is to reduce the psychiatric and physiologic barriers that keep recovery unstable.
That may involve:
- Withdrawal support: In detox, medications may be used to manage withdrawal safely and reduce medical risk.
- Psychiatric stabilization: Anxiety, depression, trauma-related symptoms, or bipolar-spectrum features may need targeted treatment.
- Medication review: Existing prescriptions are assessed for benefit, misuse risk, interactions, and whether they still fit the clinical picture.
For professionals, this step often brings relief. Many have been overmedicated, undermedicated, or prescribed without a full addiction-aware psychiatric evaluation. A good team recalibrates, rather than adding more.
The best medication plan is often the simplest one that reliably supports stability, sleep, cognition, and engagement in therapy.
Adjunctive care with a real clinical purpose
In a well-built luxury program, adjunctive therapies aren't decorative. They're used to restore capacities that work stress and substance use have eroded.
Consider how they function clinically:
- Mindfulness and meditation: Useful for nervous system downshifting, urge surfing, and interrupting compulsive mental loops.
- Fitness and movement: Help regulate mood, improve sleep, and rebuild a nonchemical relationship to stress relief.
- Somatic work: Helps clients who understand their history intellectually but still carry activation, numbness, or hypervigilance in the body.
- Art, music, or equine work: Can reach emotional material that stays inaccessible in purely verbal treatment.
For analytical clients, the turning point often comes when treatment stops feeling abstract. It becomes a daily laboratory. A triggering phone call, a shame spiral after a mistake, or the impulse to numb after conflict gets examined in real time. That's where mental health and substance abuse treatment becomes effective. Not in theory, but in repeated practice under skilled clinical supervision.
The Executive Treatment Experience Redefined
Most working professionals delay residential care for one reason above all others. They assume treatment requires disappearing completely. For a founder, physician, attorney, investor, or C-suite executive, that can feel impossible.
That assumption is one reason program design matters. Nationally, only 24% of substance use treatment facilities offer residential care, and average capacity is just 34 beds per 100,000 people, according to KFF's analysis of treatment facility availability. Limited supply means many settings aren't built for privacy, flexibility, or high-acuity dual-diagnosis work.
Why luxury features are clinically relevant
In this setting, private rooms aren't just amenities. They reduce stimulation, support confidentiality, and give professionals space to decompress after difficult psychiatric work. That matters in both detox and residential treatment, when sleep, regulation, and a sense of personal safety influence everything else.
Electronics access can also be clinically appropriate when handled with boundaries. For the right client, access to a phone or laptop allows continued oversight of urgent business matters, communication with key stakeholders, and preservation of professional continuity. That can remove a major barrier to admission.
This is especially important for clients who would otherwise postpone care until damage becomes undeniable. If treatment can accommodate limited, structured work engagement, many professionals are willing to enter sooner.
What a better-fit executive program looks like
Not every residential environment is suitable for someone carrying substantial responsibility. Executives usually need a program that can do all of the following at once:
- Protect privacy: Admission, treatment participation, and communications should be handled discreetly and professionally.
- Support complexity: Psychiatric care has to move beyond simple symptom labels and address trauma, mood, anxiety, sleep, personality patterns, and substance use together.
- Allow selective work continuity: Critical obligations can be managed without allowing work to dominate treatment.
- Match the client's pace: Intelligent, skeptical clients often engage best when the staff can explain the rationale behind each clinical intervention.
A program built for working professionals in treatment recognizes that career preservation isn't separate from recovery. For many clients, it's part of recovery. Financial stability, reputation management, leadership transitions, and ethical handoffs all influence whether a person can fully commit to care.
The trade-off that needs honest discussion
There's one important caution. Electronics access should never turn residential care into remote overwork from a nicer room. If clients spend the day inside crisis emails, market volatility, personnel disputes, and constant messaging, treatment loses potency.
The right approach is structured flexibility. Necessary contact is allowed. Nonessential re-immersion is limited. The team helps the client distinguish responsibility from compulsion.
One private-pay option in this category is Reflections, a California-licensed, Joint Commission-accredited residential program that provides dual-diagnosis care, private rooms, clinically managed detox, and appropriate access to electronics for adults who need treatment without complete professional disengagement. For the right client, that model answers the central fear that getting help will automatically derail a high-stakes career.
Building a Foundation for Lifelong Recovery
Residential treatment is where stabilization begins. Long-term recovery is built in the handoff back to real life. For executives, that transition needs more than a discharge packet and good intentions.
Many professionals return to the same pressures that shaped the problem in the first place. Travel resumes. Access returns. Social drinking culture reappears. Old relational tensions surface at home. If the recovery plan doesn't account for those realities, treatment can remain emotionally meaningful but functionally incomplete.
Family work means more than family of origin
For this population, “family” should be understood broadly. It may include a spouse, partner, adult child, parent, sibling, or another trusted support person. In some cases, a key business partner or long-time advisor also plays a meaningful stabilizing role, though clinical boundaries need to stay clear.
Effective family involvement usually focuses on three tasks:
- Clarifying the underlying problem: Loved ones often understand fragments. They may see the drinking, but not the depression, or they may focus on stress and miss the addiction component.
- Changing interaction patterns: High-functioning clients often live inside cycles of secrecy, overfunctioning, conflict avoidance, or rescue.
- Building a home environment that supports recovery: This includes communication plans, expectation setting, and practical decisions around travel, social events, or medication oversight.
Recovery is stronger when the household stops reacting only to visible behavior and starts understanding the drivers beneath it.
Family sessions also help correct a common mistake. Loved ones often think “things are better” the moment detox is complete or mood improves. The more durable marker is whether the person is building different responses to stress, shame, loneliness, fatigue, and success itself.
What meaningful aftercare includes
Strong aftercare is individualized, not generic. A comprehensive continuing-care plan should reflect the client's diagnosis, risk profile, work demands, relationship system, and living environment.
A solid plan may include:
| Aftercare element | Why it matters |
|---|---|
| Ongoing individual therapy | Keeps psychiatric and relational patterns from rebuilding in silence |
| Psychiatry follow-up | Monitors medication effectiveness, side effects, and diagnostic clarity |
| Recovery community involvement | Adds accountability and connection outside the treatment setting |
| Alumni programming | Helps clients stay engaged with peers who understand the transition |
| Sober or supportive housing when needed | Creates structure if home or travel environments are destabilizing |
For executives, one additional issue matters. The return to work should be planned clinically, not left to instinct. Some clients need a stepped re-entry. Others can resume quickly but with tighter guardrails around schedule, travel, and alcohol-centered events. A thoughtful program helps map those decisions before discharge, not after the first post-treatment crisis.
The objective isn't merely abstinence. It's a life that no longer requires substances to regulate mood, support sleep, blunt fear, or maintain professional identity. That takes continuity, repetition, and a support network that understands both the person and the pressures they're returning to.
How to Choose an Accredited Provider
Choosing a private-pay program should be handled like any other high-stakes decision. Reputation alone isn't enough. A polished website isn't enough. The questions need to focus on safety, clinical depth, privacy, and whether the program understands dual diagnosis in working professionals.
A peer-reviewed study identified affordability, geographic disparity, and insurance noncoverage as major barriers to care, and private treatment can bypass these system-level obstacles for immediate access, as discussed in this peer-reviewed review of barriers to treatment. For executives, speed matters. Delays often mean another quarter of deterioration, another failed promise at home, or another escalation in risk.
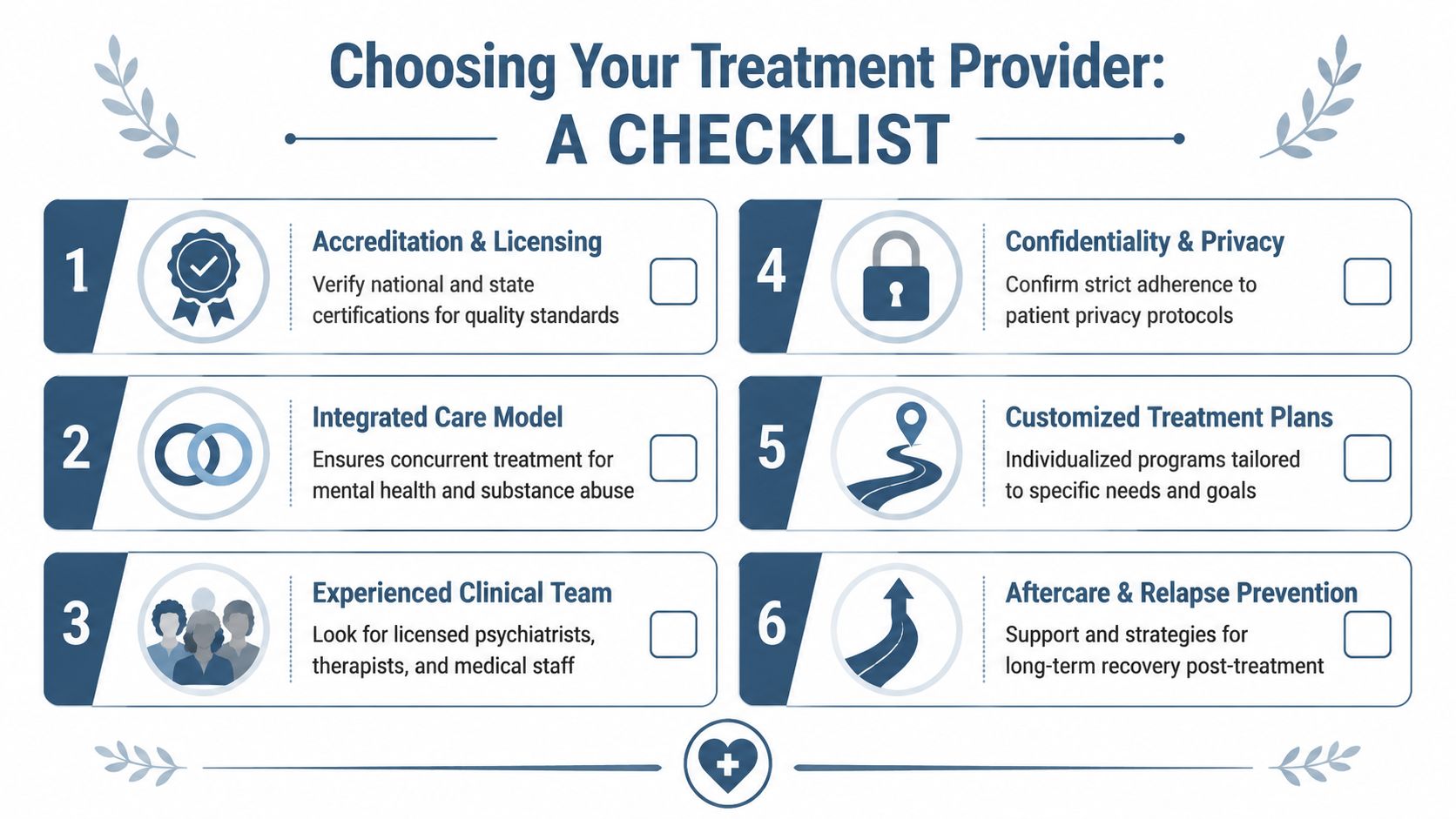
A practical checklist
When evaluating a provider, look for the following:
- Accreditation that can be verified. Joint Commission accreditation is a meaningful baseline for quality and safety. Clients who want to understand what that standard covers can review Joint Commission accreditation in treatment settings.
- A clearly integrated care model. Ask how the program treats addiction and psychiatric symptoms together. If the answer sounds split between departments, that's a concern.
- Experienced psychiatric and clinical staff. Look for licensed psychiatrists, therapists, medical personnel, and clinicians with direct experience in co-occurring disorders.
- Real confidentiality protocols. Executives should ask how communication, records, visitors, work access, and outside coordination are handled.
- Individualized treatment planning. Avoid programs that describe the same schedule and same plan for everyone.
- A defined aftercare process. Discharge planning should include psychiatric follow-up, therapy, support systems, and relapse-prevention planning.
Questions worth asking on the first call
A strong admissions or clinical conversation should be able to answer practical questions without evasion.
- How do you handle detox and psychiatric evaluation together?
- Can a client maintain limited contact with work when clinically appropriate?
- Are private rooms available in both detox and residential care?
- How is family involvement structured?
- What happens after discharge if the client travels frequently or returns to a high-pressure role?
A serious provider can explain its clinical model plainly. If the answers sound vague, scripted, or overly sales-driven, keep looking.
The right program is an investment in health, judgment, relationships, and the ability to lead without relying on substances to carry the load.
Reflections provides private-pay, accredited dual-diagnosis care for adults who need sophisticated mental health and substance abuse treatment in a discreet residential setting. For executives, founders, and other working professionals, that can include private rooms in detox and rehab, integrated psychiatric and addiction treatment, family involvement, and appropriate access to electronics so urgent career responsibilities can be managed without abandoning care. Those exploring options can learn more about Reflections.









