At 11:40 p.m., the laptop is still open, the phone is still lighting up, and the mind still hasn't stopped running. A board packet is due in the morning. Family members are asking whether treatment means disappearing from work. Part of the brain knows that alcohol, stimulants, opioids, or compulsive coping can't keep carrying this load. Another part insists that stepping away, even briefly, could cost too much.
That conflict is common among executives, founders, physicians, attorneys, investors, and other high-responsibility professionals. They don't need vague advice. They need a method that respects reality: sustained pressure, high cognitive demand, intense privacy concerns, and the need to protect judgment while rebuilding health.
That's where Meditation for recovery belongs. Not as a spa add-on. Not as a moral exercise. As a disciplined mental skill that helps a high-performing person regain control over attention, stress reactivity, pain, craving, and emotional volatility.
In a high-end residential setting designed for executives, that distinction matters. Luxury treatment isn't about excess. It's about precision, privacy, private rooms in detox and rehab, exceptionally credentialed clinical care, and enough structure to support recovery without forcing a complete severance from legitimate professional obligations. Executive programs may allow residents to retain access to electronics such as cell phones and laptops during non-treatment hours so they can maintain critical work responsibilities, while limiting use during therapy to preserve clinical focus, as described in this overview of luxury executive rehab programs.
Beyond Stress Relief An Executive's Introduction
At 11:40 p.m., the inbox is still active, tomorrow's decisions are still unresolved, and the body is sending signals the mind keeps trying to override. Sleep is shallow. Patience is shorter than it used to be. A drink, a pill, or another private coping ritual starts to serve a new function. It stops being a reward and becomes a way to regulate a nervous system that no longer resets on its own.

That is the point at which many high-performing professionals dismiss meditation too quickly. The word can sound vague, passive, or detached from realities of leadership. In clinical practice, it functions very differently. Meditation is a trained method for stabilizing attention, increasing awareness of internal cues, and interrupting automatic reactions before they become decisions with consequences.
For executives, that distinction matters.
People who succeed in demanding roles already understand practice, repetition, and disciplined execution. Meditation applies those same principles to the mind under strain. You are not trying to become less driven. You are building greater control over where attention goes, how quickly threat responses escalate, and what happens in the few seconds between impulse and action.
The benefits show up in operational moments, not abstract ideals:
- Before a high-stakes call: physical tension is noticed early enough to prevent rushed, defensive communication.
- During conflict: irritation is recognized before it hardens into contempt, blame, or a strategic mistake.
- After a trigger: craving can be observed as an event in the mind and body, rather than obeyed as an instruction.
- At night: stillness becomes more tolerable, which improves the conditions for actual rest.
Meditation does not reduce standards. It improves the internal conditions required to meet them.
What luxury treatment changes
In an executive residential setting, meditation becomes easier to adopt because the environment is built for focus, privacy, and clinical precision. The goal is not total withdrawal from adult responsibility. The goal is to reduce noise, tighten structure, and create enough protected space for the nervous system to settle while treatment proceeds at a serious level.
That changes compliance. A private room supports practice without performance or exposure. A discreet setting lowers the social friction that keeps many accomplished professionals guarded. Structured schedules, high clinician availability, and carefully managed communication with the outside world reduce resistance from clients who carry legitimate responsibilities and cannot tolerate chaos disguised as care.
There are trade-offs. Continued contact with work can lower panic in the first phase of treatment, but too much access can keep the brain in the same reactive loop that fueled the problem. Strong executive programs handle that tension directly. They do not promise constant connectivity or demand theatrical detachment. They set limits that protect treatment while accounting for reality.
Meditation fits this model because it is portable, clinically useful, and easy to integrate across the day. It can be practiced in a private room before a family session, after trauma work, or in the interval between a difficult update and an appointment with the treatment team. For a successful professional in recovery, that makes meditation more than stress relief. It becomes a strategic skill for protecting judgment, reducing relapse risk, and restoring sustainable performance.
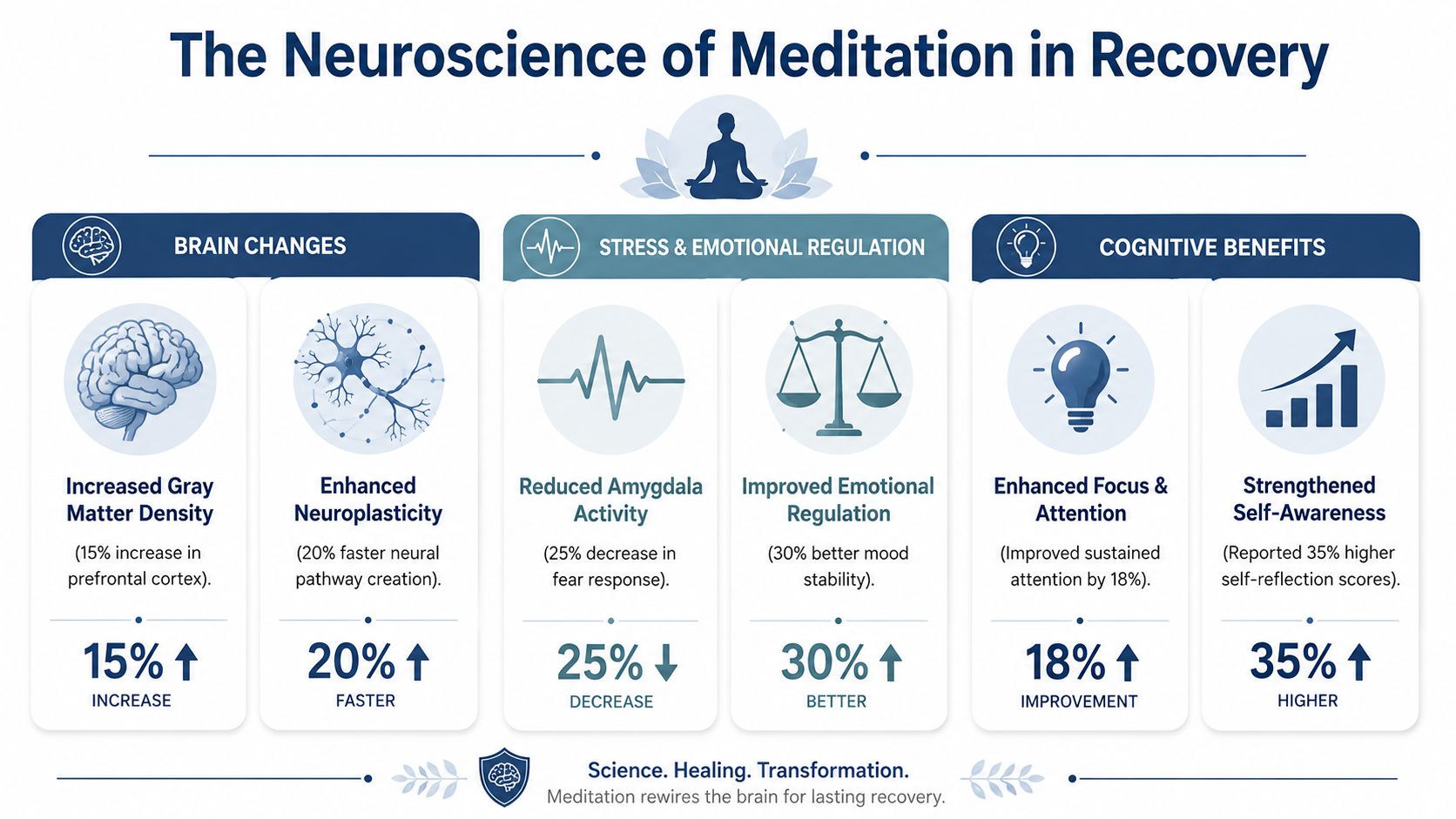
The Neuroscience of Meditation in Recovery
At 11:40 p.m., the inbox is still active, your body is tired, and your mind is running threat calculations at full speed. In that state, recovery is not usually disrupted by a dramatic decision. It is disrupted by a nervous system that has lost flexibility.
That is why meditation belongs in treatment for executives and other high-responsibility professionals. The clinical value starts in the brain. Regular practice improves attention control, lowers automatic stress reactivity, and increases awareness of internal cues before they become action.
One of the better-known early imaging studies, published in Psychiatry Research: Neuroimaging, found changes in brain regions involved in learning, memory, self-awareness, and emotional regulation after an eight-week mindfulness program. A separate review in JAMA Internal Medicine found that mindfulness meditation programs can improve anxiety, depression, and pain. The National Center for Complementary and Integrative Health has also summarized evidence linking meditation with changes in brain networks involved in attention and emotion regulation. For a client in recovery, those findings matter because treatment depends on noticing activation sooner and responding with more choice.
What that means clinically
In practice, meditation trains a sequence that many clients have not used consistently in years. Notice the signal. Stay with it long enough to name it accurately. Choose a response that does not worsen the situation.
That sequence sounds simple. Under pressure, it is not.
Substance use disorders narrow attention, amplify urgency, and reduce tolerance for discomfort. High performers often compensate for that deterioration for a long time. They keep producing, keep deciding, and keep carrying responsibility. The cost shows up elsewhere, in sleep, irritability, pain, compulsive thinking, and the familiar pattern of using something fast to shut the system down. Meditation helps restore the gap between impulse and action, which is one of the most useful capacities we try to rebuild in treatment.
A practical way to frame the mechanism is below:
| Domain | What meditation trains | Why it matters in recovery |
|---|---|---|
| Attention | Returning to one anchor after distraction | Interrupts compulsive mental loops |
| Interoception | Detecting body cues earlier | Identifies stress, craving, and escalation sooner |
| Emotion regulation | Staying present without immediate discharge | Reduces impulsive decisions |
| Metacognition | Observing thought as thought | Weakens automatic identification with urges |
Pain, craving, and executive function
Many clients entering treatment are dealing with more than alcohol or drug use. They may also have chronic pain, insomnia, stimulant-driven depletion, or the physiological wear of sustained overwork. Those conditions increase relapse risk because pain and exhaustion reduce judgment and make short-term relief look rational.
Mindfulness-based approaches have shown benefit for both pain and substance-related outcomes, including work led by researchers studying Mindfulness-Oriented Recovery Enhancement. I discuss meditation in this context with clients as a performance protection tool, not as a soft add-on. If a practice lowers reactivity, improves pain tolerance, and gives a person a better chance of pausing before acting on an urge, it has direct clinical value.
The trade-off is time and consistency. Meditation does not produce the same immediate effect as a sedative, a drink, or a familiar compulsive behavior. It asks for repetition before the return shows up under pressure. For successful professionals, that can be the hardest part. They are used to interventions that produce visible results quickly. Meditation works more like conditioning. The gains are gradual, then suddenly very practical in a meeting, after a difficult call, or during a spike in craving.
That is also why setting matters. In a structured clinical environment, meditation is easier to apply with discipline and less guesswork. Our mindfulness-based treatment approach at Reflections uses these practices as part of a broader plan that includes medical oversight, psychotherapy, and careful pacing. Some clients also find that environmental cues support consistency. For example, controlled sensory rituals such as using incense for mindfulness can help mark the transition into practice, provided they are used intentionally and fit the treatment setting.
For a data-driven mind, the conclusion is straightforward. Meditation improves the brain functions that addiction, chronic stress, and sleep disruption tend to impair first: attention, self-regulation, and the ability to pause. In recovery, that is not abstract. It is the difference between reacting automatically and making a decision you can still respect the next morning.
Foundational Practices for a Disciplined Mind
At 6:30 a.m., before the first call of the day, many executives can generate ten plans, three contingencies, and a polished explanation for why they are fine. What they often cannot do, at least early in recovery, is sit still for five minutes without their mind sprinting toward the next demand or the next escape. That is the training problem meditation addresses.
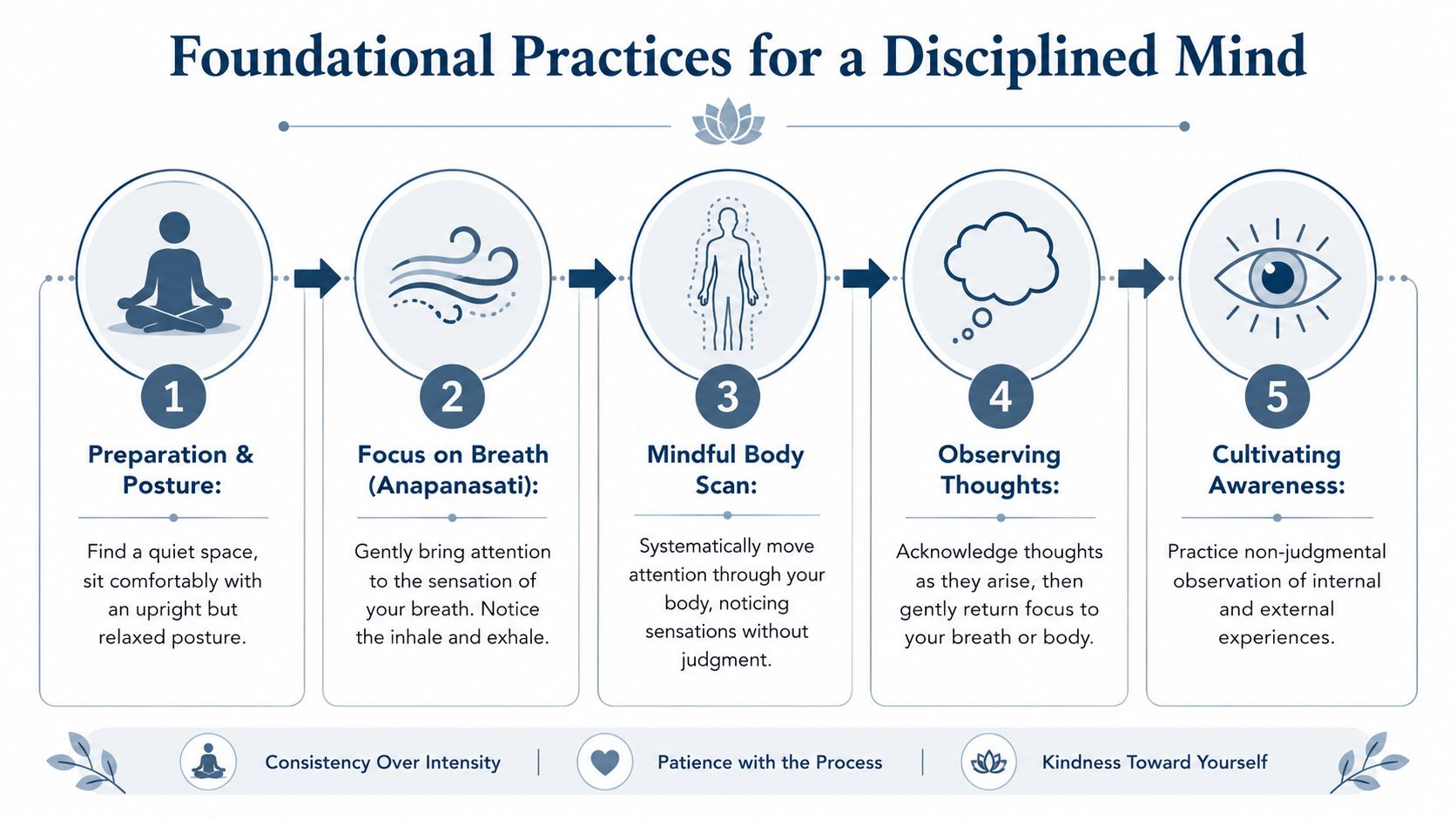
The starting point should be disciplined, brief, and repeatable under real conditions. In clinical work, I usually begin with three practices: focused breathing, body-based awareness, and urge observation. Each trains a different capacity that high-functioning professionals need in recovery. Attentional control, accurate self-monitoring, and the ability to pause before acting.
Focused breathwork for immediate stabilization
Breath practice is often the best entry point because it is discreet and portable. It can be used in a private office, in a treatment setting, or after a difficult conversation when the nervous system is already accelerating.
Sit upright without bracing. Put both feet on the floor if you are in a chair. Rest your hands. Then choose one physical sensation of breathing to follow, such as air moving at the nostrils or the rise of the chest.
The assignment is narrow on purpose. Notice the inhale. Notice the exhale. When attention leaves, return it.
A practical sequence looks like this:
- Set the posture: stable, supported, eyes open or softly lowered.
- Choose one anchor: nostrils, chest, or abdomen.
- Use counting briefly if needed: then drop it once attention settles.
- Return each time the mind wanders: that return is the repetition that builds control.
Clients in early recovery often mistake internal speed for readiness. They feel charged and call it focus. Breathwork helps separate activation from clarity, which matters when a fast decision could also be a reckless one.
The body scan for reconnection
Many senior professionals are rewarded for living cognitively. They can read a room, make a decision under pressure, and manage consequences quickly while missing basic physical signals such as fatigue, jaw tension, shallow breathing, or the flat heaviness that often shows up before a lapse in judgment.
That gap creates risk.
A body scan rebuilds contact with those signals. It teaches observation before interpretation, which is a useful correction for people who are used to analyzing everything before they have felt it.
Try this sequence:
- Start at the feet: notice pressure, temperature, tingling, or numbness.
- Move upward in order: calves, thighs, pelvis, abdomen, chest, shoulders, jaw.
- Label sensation rather than explanation: tight, warm, restless, heavy.
- Leave relaxation out of the goal: first notice what is present. Change may follow later.
The trade-off is straightforward. A body scan can feel unproductive to someone who prefers visible progress and quick resolution. In practice, it often improves performance because it catches overload early, before it appears as irritability, impulsivity, or a craving that seems to come out of nowhere.
For some clients, a controlled sensory cue helps mark the transition from work mode to practice without turning the ritual into a dependency. That is one reason some people experiment with using incense for mindfulness, provided the cue stays simple and clinically appropriate.
Mindfulness of urges without obeying them
Urges rarely arrive as polite suggestions. They come with momentum. For executives, that momentum can pair with a professional reflex to act quickly, solve the problem, and move on. That trait builds careers. It can also shorten the space between craving and behavior.
Urge observation trains a different response. The goal is not to argue with the craving or crush it by force. The goal is to notice it precisely enough that it stops functioning like an order.
A short protocol looks like this:
| Step | What to do | What to avoid |
|---|---|---|
| Name it | “Urge is present” | “I have to get rid of this now” |
| Locate it | Notice where it sits in the body | Turning it into a debate |
| Track change | Observe whether it rises, plateaus, or drops | Assuming intensity means permanence |
| Return to anchor | Use breath or posture to stabilize | Chasing relief through action |
This matters for more than substance craving. The same skill helps with the urge to leave treatment emotionally, overwork, pick a fight, isolate, or reach for any familiar behavior that promises immediate relief and creates a larger problem by tomorrow morning.
Making the practice fit a full schedule
Meditation has to survive contact with a real calendar. If a practice only works in perfect silence with unlimited time, many successful professionals will abandon it the first week they return to responsibility.
Short sessions done consistently work better. Five minutes before messages. Three minutes after a tense family call. Ten minutes after psychotherapy, when the mind is looking for a fast exit. In residential care, that rhythm is easier to establish because the structure supports repetition and accountability. Clients who want to see how these skills are taught inside a clinically managed setting can review the mindfulness-based treatment approach at Reflections.
The standard is not a pristine meditation routine. The standard is a trained mind that can recover its footing under pressure.
Navigating Complex Emotions with Trauma-Informed Practice
At 2 a.m., a senior executive finally has a quiet moment, tries a standard meditation app, closes their eyes, and within seconds feels trapped, agitated, or flooded by memory. In recovery, that reaction matters. It changes how meditation should be prescribed.
Meditation is not universally calming. For clients with trauma histories, dissociation, PTSD symptoms, bipolar spectrum features, or severe anxiety, inward attention can intensify distress. A quiet room can lower stimulation for one person and increase threat for another. In clinical practice, I treat that response as useful data about nervous system tolerance, not as lack of motivation.
That is why meditation in recovery has to be trauma-informed and clinically managed.
When stillness activates the nervous system
A client may follow perfectly reasonable instructions, focus on the breath, and become overwhelmed within a minute. Another may go numb, lose a sense of time, or feel detached from the room. Some become hypervigilant. Others are pulled toward intrusive images, shame, or panic.
These are not rare edge cases in an executive treatment setting. High-functioning professionals often arrive with years of compartmentalization, chronic overcontrol, sleep disruption, stimulant or alcohol use, and unresolved trauma that was masked by performance. Silence removes distractions. It also removes defenses.
Generic mindfulness guidance often assumes that more observation is always better. In trauma treatment, that assumption fails. The task is to regulate arousal first, then widen awareness as capacity improves. Clients who want a clearer picture of how this is handled in treatment can review our approach to trauma-informed therapy.
Safety rule: If a practice increases panic, disorganization, dissociation, or re-experiencing, change the method, shorten the exposure, or stop and reassess.
What trauma-sensitive meditation looks like in practice
The goal is not passive endurance. The goal is enough stability to stay present without becoming flooded.
That often means giving the client more control over the exercise. Eyes may stay open. Attention may rest on the room rather than the body. Sessions may last two minutes instead of twenty. A clinician may choose movement, sound, or visual orientation before any breath-focused work. For some clients, the first useful meditation practice is a slow walk with deliberate attention to foot pressure, posture, and the environment.
Common modifications include:
- Eyes-open grounding: orienting to the room, identifying shapes, colors, light sources, and exits.
- Movement-based practice: walking, stretching, or paced movement that keeps attention anchored in the present.
- External points of focus: sound, texture, temperature, or a fixed visual object instead of internal sensation.
- Limited-dose body awareness: noticing contact with the chair or feet on the floor before approaching stronger sensations.
- Choice-based pacing: stopping, shifting anchors, or shortening the exercise the moment activation rises too far.
Compassion-based practices can help, but timing matters. A client with severe shame or trauma may not tolerate phrases directed toward the self at first. In those cases, we start with a neutral person, a pet, or a simple focus on safety and steadiness. The trade-off is slower progression, but the work is more stable and far less likely to trigger avoidance.
What tends to go wrong
Three mistakes repeatedly undermine this work.
- Using one standard protocol for everyone. Silent breath awareness is effective for some people and destabilizing for others.
- Confusing intensity with progress. A strong emotional reaction may reflect activation, not therapeutic gain.
- Treating meditation as separate from treatment. For clients with trauma and substance use disorders, meditation has to be coordinated with psychotherapy, psychiatric care, sleep stabilization, and relapse-prevention planning.
In a well-run residential program, meditation is selected the way any other intervention is selected. It has an indication, a dose, a timing strategy, and clear reasons to modify it. That is how it becomes both safer and more useful for people whose careers trained them to override internal warning signs for years.
Integrating Meditation into a Residential Program
At 6:30 a.m., before the first confidential call, market update, or family request, the mind often shows its real condition. For many executives in treatment, that moment is not calm. It is speed, scanning, and the reflex to get ahead of the day before the body has even settled. In residential care, meditation is built into that exact pressure point. It is used as a clinical intervention that improves regulation, attention, and follow-through across the rest of treatment.
Regular practice matters more than intensity. In recovery, the clients who benefit most are rarely the ones doing long, impressive sessions a few times and then disappearing for a week. The ones who gain traction are the people who practice on a repeatable schedule, with methods matched to their symptoms and enough clinical support to adjust quickly when the practice stops helping.
Why residential structure matters
A residential setting gives clients something home routines usually do not. Protected repetition.
That matters because meditation in recovery works best when it is attached to predictable moments in the day. We often place shorter sessions before psychotherapy, after emotionally demanding groups, during late afternoon stress peaks, and in the evening when agitation, craving, or mental overdrive can build. The point is not to fill the schedule with wellness activities. The point is to lower the number of hours in which a client is operating on reflex.
For high-responsibility professionals, structure also solves a practical problem. Many have spent years performing well while chronically dysregulated. They can close deals, manage teams, and carry large amounts of risk while missing early signs of exhaustion, resentment, or urge escalation. A residential schedule interrupts that pattern often enough for new awareness to become usable, not theoretical.
Individual sessions and group practice serve different functions
These formats are not interchangeable.
Individual meditation sessions allow precise tailoring. A client with stimulant use and severe sleep disruption may need brief grounding practices that reduce activation rather than extended silent sitting. A client with alcohol dependence and high workplace stress may benefit more from urge surfing timed to the evening window when cravings usually increase. Another may need a two-minute reset that can later be used discreetly between board calls or legal meetings.
Group meditation adds a different type of value. It reduces the isolation that high achievers often bring into treatment. It also exposes a useful truth. Restlessness, skepticism, boredom, and resistance are not signs that someone is failing at meditation. They are common observations that can be named, monitored, and worked with. In group settings, clients also see how disciplined practice looks in real time, which improves adherence more effectively than abstract encouragement.
Where it fits for working professionals
Meditation should support the rest of the treatment plan. In practice, that means it is coordinated with psychotherapy, psychiatric care, sleep restoration, physical health goals, and relapse-prevention work. A client who notices rising arousal earlier can use CBT or DBT skills with better timing. A client who can remain present for ninety seconds longer during discomfort is often less likely to react automatically with avoidance, anger, or craving.
The trade-off is straightforward. Clients do not get to use meditation as a polished self-optimization ritual while ignoring the harder parts of treatment. They also should not be pushed into practices that look impressive on paper but leave them overstimulated, detached, or less able to engage in therapy. Good clinical integration requires selection, timing, review, and modification.
For professionals who still need to contain limited outside responsibilities, the setting has to protect treatment without pretending real life has disappeared. Programs designed for residential treatment for adults can combine privacy, clinical intensity, and clear boundaries around communication, so clients can address necessary obligations without handing the day back to work. That level of precision is what makes meditation useful in executive recovery. It becomes a disciplined support for judgment, emotional control, and sustainable performance.
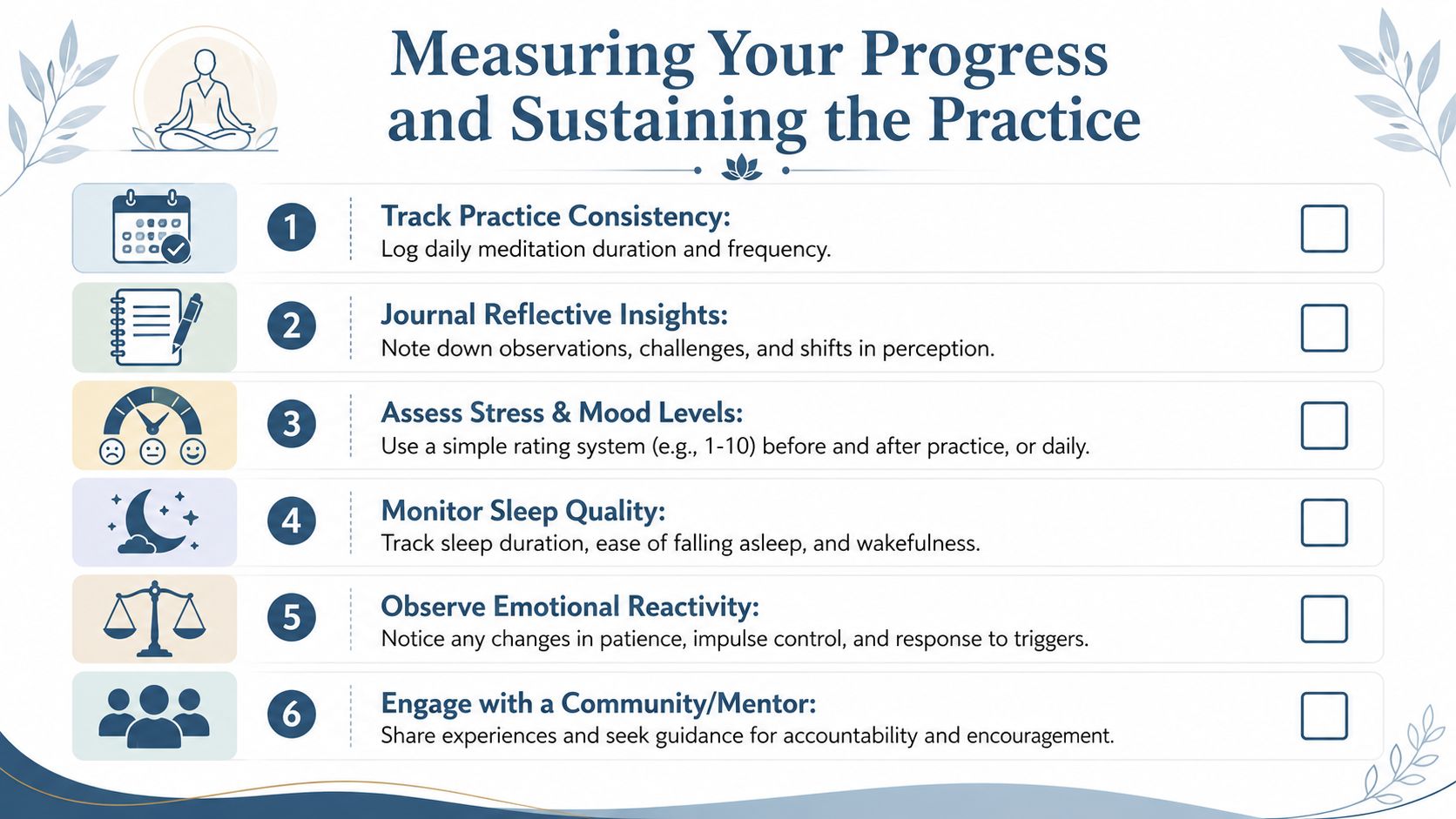
Measuring Your Progress and Sustaining the Practice
High-performing people usually stay committed when they can observe movement. Meditation shouldn't be treated as a leap of faith. It should be tracked like any other recovery intervention.
New developments reported for 2025 indicate that measurable reductions in relapse risk typically occur after 6 to 8 weeks of daily practice, with a minimum of 20 minutes, and that a 2025 cohort study in Addiction Biology reported a 22% drop in illicit substance use. That timeline helps answer the practical question most professionals ask first: when should results start to show up?
What to track
The best measurement system includes both subjective and behavioral markers. It doesn't need to be complicated. It does need to be consistent.
A practical scorecard might include:
- Practice consistency: log whether the session happened, how long it lasted, and what type was used.
- Anxiety and mood: use a brief self-report measure such as OASIS, or even a simple daily rating scale.
- Physiological regulation: track heart rate variability or other clinician-approved biomarkers if available.
- Sleep quality: note time to fall asleep, night waking, and morning alertness.
- Relapse indicators: record urges, near-misses, and actual substance use episodes without sanitizing them.
How to read the data
Meditation is working when the client sees changes such as faster recovery after stress, fewer impulsive reactions, more awareness before craving peaks, and better use of therapeutic skills under pressure. The first sign usually isn't bliss. It's increased notice.
That distinction matters. Early progress often looks like, “The urge was still there, but it didn't run the meeting.” That's a major gain.
Progress in meditation for recovery is often visible before it feels impressive.
Keeping it alive after residential care
The most durable post-treatment practices are simple enough to survive travel, work intensity, and imperfect days. A strong maintenance plan usually includes a fixed daily time, one fallback micro-practice for overloaded days, periodic clinical or peer accountability, and a rule that missed sessions don't turn into abandoned weeks.
For executives, sustainability also depends on environment. A quiet chair in a home office, a short pause before opening email, or a reset after commuting can become reliable anchors. The point isn't to create a perfect ritual. It's to create a repeatable one.
Reflections provides California-licensed, Joint Commission-accredited luxury dual-diagnosis care for adults who need serious treatment without sacrificing privacy, clinical sophistication, or the realities of a high-responsibility life. With private rooms in both detox and residential rehab, highly individualized treatment, and appropriate access to electronics so clients can remain connected to essential work obligations, the program is built for executives, C-suite leaders, and other professionals who need the best of the best in discreet private-pay care. Those exploring whether meditation, trauma-informed treatment, and extensive residential support belong in the same plan can learn more at Reflections.









