A managing partner closes the laptop at midnight, then opens it again at 2 a.m. A founder snaps at a spouse over nothing, then walks into a board meeting polished and composed. A physician starts relying on alcohol, pills, or sheer force of will to keep performing while anxiety, depression, trauma, or exhaustion insidiously start running the show.
That profile is common in high-performing adults. Outward success hides internal instability well, until it doesn't. For executives, C-suite leaders, attorneys, physicians, investors, and other high-earning professionals, the primary barrier usually isn't recognizing that something is wrong. It's fearing that treatment will damage privacy, reputation, income, or momentum.
That fear keeps people stuck in partial solutions. They try a weekly therapist while continuing the same punishing schedule. They white-knuckle it through panic, insomnia, irritability, and substance misuse. They call it stress management when it is deterioration.
Residential mental health care, at the executive level, should be understood differently. It isn't an exile from life. It's a protected, clinically advanced environment where serious work gets done without forcing a successful person to torch a career in the process.
Recognizing the Need for Comprehensive Support
A high-functioning executive rarely looks “sick” from the outside. Performance often remains intact long after peace, sleep, focus, and emotional steadiness have collapsed. The calendar stays full. Deals still close. The family still hears, “Everything's under control.”
It usually isn't.

A common pattern looks like this: a leader starts waking up tense, needing alcohol or medication to slow the mind at night, and becoming more reactive with colleagues or family. Attention narrows. Judgment gets less flexible. Shame grows because the person who can solve everyone else's problems can't seem to solve this one. Many of the hidden signs of addiction in executives are easy to rationalize until the cost becomes obvious.
When success starts masking decline
Mental health strain at this level rarely presents as dramatic collapse first. It presents as overcontrol, isolation, cynicism, compulsive working, emotional blunting, and escalating self-medication. The person still shows up. The person stops feeling like himself or herself while doing it.
Globally, the scale of need is enormous. Over 1 billion people are living with mental health disorders, and anxiety and depression remain the most prevalent across countries and income levels. These conditions are also the second largest cause of long-term disability worldwide, and suicide claims an estimated 727,000 lives annually. The economic toll is about $1 trillion each year in lost productivity, even while median government spending on mental health remains 2% of total health budgets. Spending disparities are stark, from up to $65 per person in high-income countries to as little as $0.04 in low-income countries, according to the World Health Organization's 2025 mental health report.
The strongest professionals often wait too long because they mistake endurance for stability.
Why residential care becomes the right call
For an executive, extensive support becomes necessary when outpatient care can't create enough distance from triggers, obligations, and patterns that keep the problem alive. If symptoms are persistent, if substance use is involved, if trauma keeps surfacing, or if function depends on constant compensation, a higher level of care is the disciplined move.
Residential mental health treatment is not a retreat for people who've failed. It's a strategic intervention for people whose lives are too important to keep managing in survival mode.
Defining Executive Residential Mental Health Care
Executive residential mental health care is a 24/7 live-in treatment setting built for adults who need depth, discretion, and real clinical structure. It is not a hospital ward. It is not a punishment model. And it should never feel like a generic program built for the broadest possible audience.
A better comparison is a high-performance training camp for mental wellness. Daily life is structured on purpose. Therapy is intensive. Assessment is deeper. Patterns become visible because the noise of ordinary life is reduced enough for real work to happen.
What it is and what it isn't
Traditional assumptions about rehab still mislead professionals. Many imagine locked doors, confiscated devices, little autonomy, and a total break from career responsibilities. That old picture is one reason executives delay care.
The modern executive model looks different:
- Immersive care: Clients live in a therapeutic environment where clinicians can observe patterns, adjust treatment, and respond quickly.
- Root-cause treatment: Work focuses on trauma, anxiety, depression, burnout, substance use, grief, relational conflict, and the habits that sustain them.
- Protected privacy: The setting is designed to reduce exposure, preserve confidentiality, and give clients room to stabilize without public scrutiny.
- Functional integration: Family contact, selected work obligations, and future planning are handled deliberately rather than ignored.
Why executives need a different design
Most residential programs don't work for high-responsibility professionals. Data from Colorado HCPF shows that 92% of standard facilities ban electronics entirely, which is a direct barrier for anyone who must maintain oversight, communication, or limited operational involvement while in care, as noted by the Colorado Department of Health Care Policy and Financing.
That detail matters more than many marketing claims about “comfort.” Electronics access isn't a luxury add-on for a CEO, managing director, physician, or business owner. It can be the difference between entering treatment now and postponing it until a crisis forces the issue.
Practical rule: If a program can't clearly explain how it handles phones, laptops, urgent work communication, and confidentiality, it isn't built for executives.
What the day is meant to accomplish
Executive residential treatment should help a client do three things at once:
- Stabilize clinically so sleep, mood, anxiety, and substance-related symptoms stop dictating daily function.
- Build durable skills for stress, boundaries, emotion regulation, and decision-making under pressure.
- Return with a plan that makes professional success sustainable instead of self-destructive.
Good residential mental health care doesn't ask a professional to abandon real life. It teaches that person how to re-enter real life with more judgment, more capacity, and far less hidden chaos.
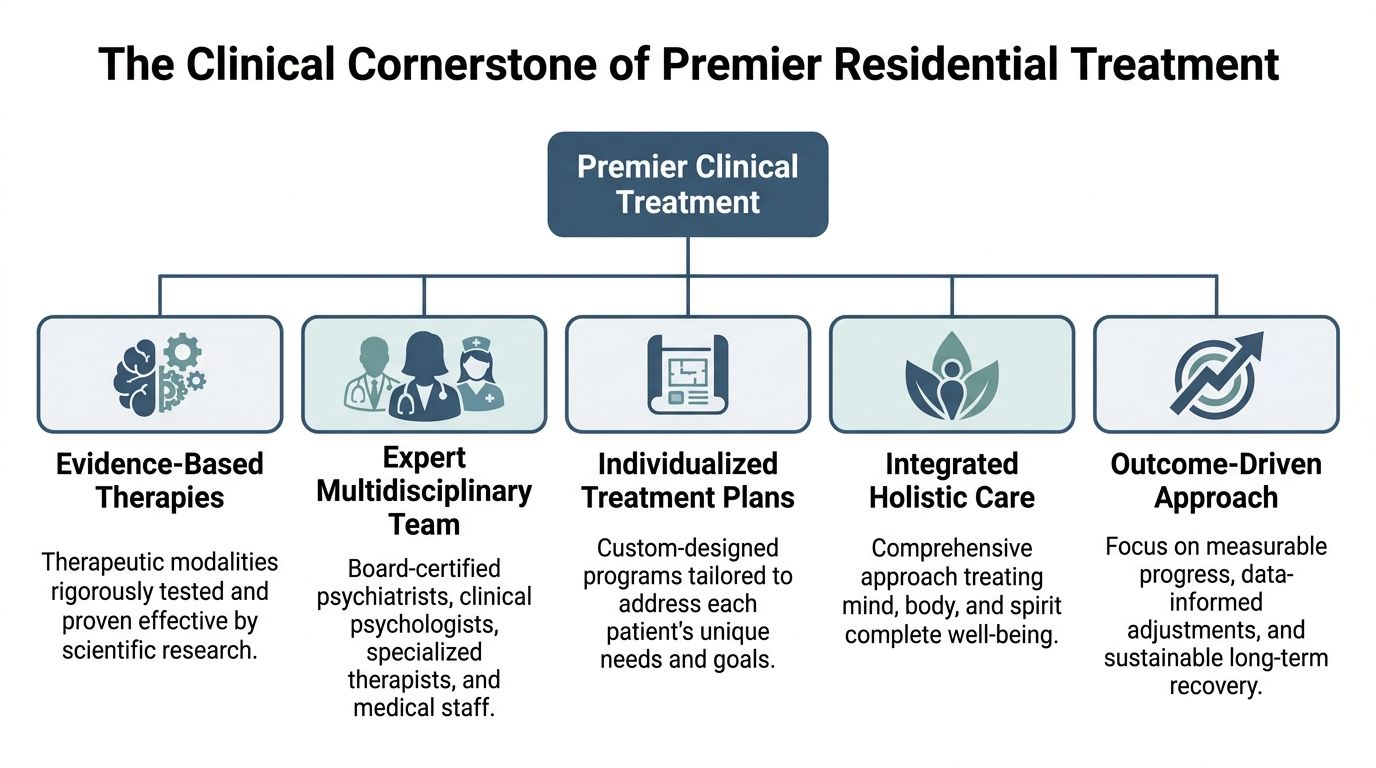
The Clinical Cornerstone of Premier Treatment
High-end surroundings are irrelevant without high-level clinical substance. Executives don't need prettier dysfunction. They need a program with the depth to diagnose accurately, treat co-occurring conditions correctly, and adapt care as new information emerges.
That starts with accreditation, credentialed leadership, and a treatment team that can do more than offer supportive conversation.
Dual diagnosis is not optional
Many executives present with both mental health symptoms and substance use. Anxiety feeds drinking. Trauma drives stimulant misuse. Depression leads to sedative dependence. Treating one while minimizing the other is sloppy medicine.
The benchmark to verify is dual diagnosis capability. National data indicates that only about 9% of mental health programs and 18% of addiction programs are equipped to be “Dual Diagnosis Capable,” according to this research on co-occurring disorder capability. That scarcity means most programs are not prepared to handle complex overlap well.
A client evaluating residential mental health options should ask direct questions:
- Assessment depth: Does the program evaluate psychiatric symptoms and substance use together from day one?
- Medication oversight: Is psychiatric prescribing integrated with addiction treatment, detox planning, and symptom monitoring?
- Discharge planning: Does the team prepare continuity of care for both sides of the diagnosis, not just one?
What strong clinical treatment looks like
A premier program should provide more than nice language about personalization. It should demonstrate it through staffing, treatment planning, and measurable decision-making. A useful starting point is to review how a provider approaches personalized treatment planning before admission.
The clinical essentials should include:
- Joint Commission accreditation: Accreditation reflects systems, oversight, and accountability. For discerning clients, that's a baseline, not a bonus.
- A multidisciplinary team: Psychiatrists, psychologists, licensed therapists, nursing staff, and addiction clinicians should work from one integrated plan.
- Evidence-based therapies: Cognitive and behavioral treatments teach practical responses to stress, distorted thinking, impulsivity, avoidance, and emotional volatility.
- Trauma-informed care: Many high achievers are organized around unresolved trauma. If a program treats symptoms without addressing that substrate, progress won't hold.
- A high-touch environment: Frequent clinical contact gives staff the chance to adjust quickly when someone is overperforming, underreporting, or intellectually bypassing the work.
How to separate clinical depth from polished marketing
There's another nuance executives should understand. Integrated treatment for co-occurring disorders does improve psychiatric symptomatology, particularly PTSD and depressive symptoms, but evidence is mixed on whether integrated models always outperform non-integrated treatment on retention and substance misuse outcomes. A systematic review of 11 studies found stronger reductions in psychiatric hospitalization and arrest frequency in some integrated approaches, while retention differences were not consistently significant, according to this systematic review on integrated treatment.
That finding doesn't weaken the case for integrated care. It sharpens it. Program structure, cultural fit, and engagement quality matter alongside the model itself.
A sophisticated program doesn't just offer therapy. It knows how to keep accomplished, defended, skeptical adults engaged long enough for therapy to work.
For clients who respond to experiential work alongside formal therapy, reflective resources can also help families and professionals understand why nontraditional approaches matter. This therapeutic horsemanship book offers a thoughtful look at healing through relational and experiential practice.
One example in this category is Reflections, a California-licensed, Joint Commission-accredited residential provider for adults with co-occurring mental health and substance use disorders, offering private-pay treatment with PhD-level psychologists, psychiatrists, private rooms, electronics access, and clinically managed sub-acute detox when appropriate.
Residential Care vs Other Levels of Treatment
Choosing the wrong level of care wastes time, money, and momentum. The question isn't which option sounds least disruptive. The question is which option matches the actual severity, complexity, and relapse risk in front of the client.
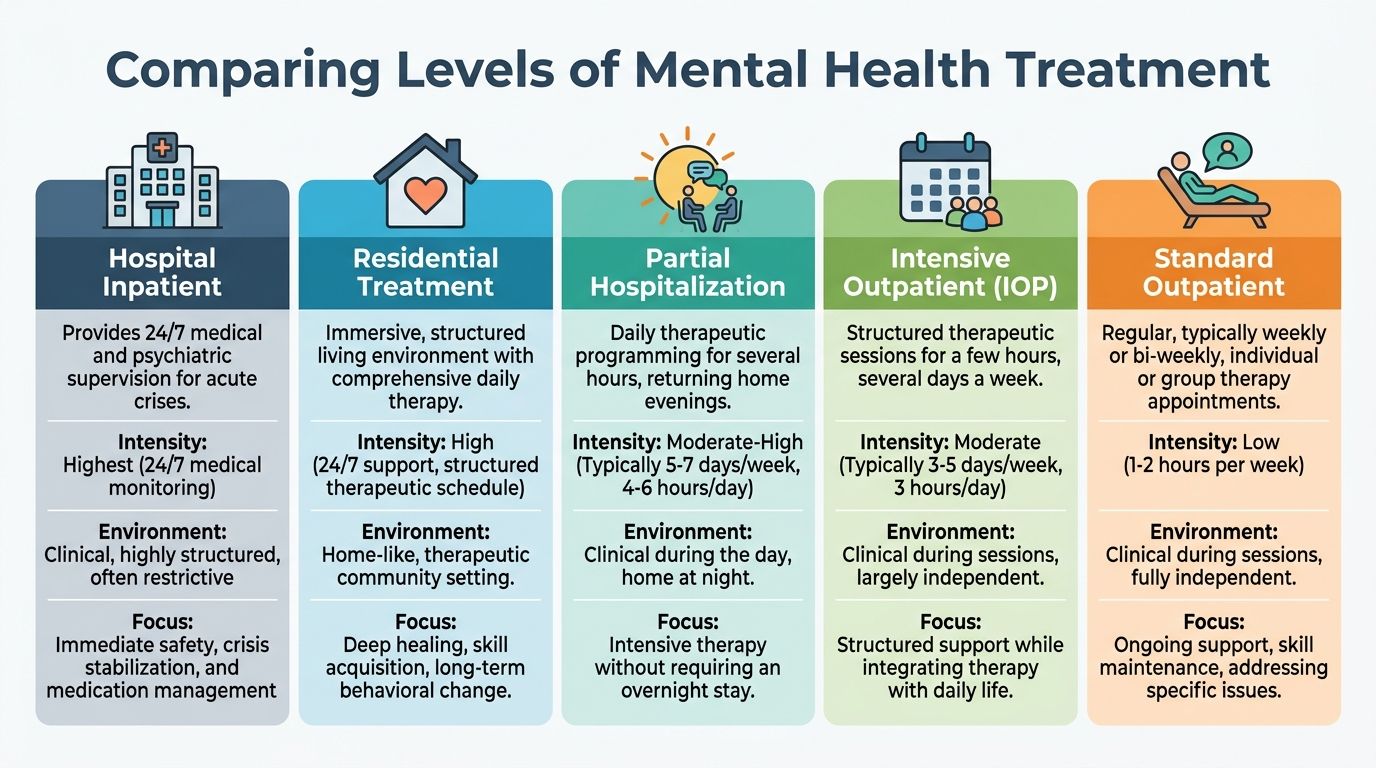
Hospital inpatient, residential, PHP, and IOP all have a place. They just do different jobs.
The right tool for the right problem
| Level of care | Best use | Limitation for executives |
|---|---|---|
| Hospital inpatient | Acute crisis, safety concerns, medication stabilization | Too short and medically focused for deeper behavioral and relational work |
| Residential mental health | Complex mental health issues, dual diagnosis, persistent dysfunction, need for immersive change | Requires stepping out of ordinary routines long enough to do serious work |
| PHP | Strong step-down support with daily programming | Client still returns home each evening, where stressors and access to substances remain |
| IOP | Structured support while maintaining broader independence | Often insufficient when the home or work environment keeps destabilizing the person |
| Standard outpatient | Maintenance, targeted therapy, long-term follow-up | Too light for someone already losing control underneath high performance |
Why residential often makes more sense than inpatient
Hospital inpatient care is designed for crisis stabilization. It protects safety, manages acute symptoms, and gets someone out of immediate danger. That is necessary in the right moment, but it is rarely enough for an executive whose problems have been building for months or years.
Residential care is where meaningful repair happens. It creates enough time and structure to identify patterns, interrupt substance use, address trauma, recalibrate medication if needed, and train new coping responses before discharge.
That difference shows up in outcomes. Residential treatment yields 42% lower 12-month relapse rates for co-occurring disorders compared to shorter inpatient stays, according to the American Society of Addiction Medicine. Upfront cost is higher, but short-term savings mean little if the person is back in crisis after discharge.
Short stabilization is valuable. Sustained recovery requires enough time for behavior, nervous system patterns, and daily habits to actually change.
Where PHP and IOP fit
PHP and IOP are often strong options after residential treatment. They help clients practice recovery skills with increasing independence while preserving clinical accountability.
They are weaker starting points when an executive is still surrounded by daily triggers, active substance use, severe burnout, uncontrolled anxiety, or concealed psychiatric instability. In those cases, asking outpatient levels to do residential work usually fails.
For high-functioning professionals with complex presentations, residential mental health is often the most efficient route because it stops the cycle of under-treating a serious problem.
Accommodations for the Demands of a Career
For high-earning professionals, so-called luxury features are usually operational necessities. A private room isn't just comfort. It protects confidentiality, allows decompression, and makes a sensitive call possible without turning treatment into a spectacle.
The same is true for electronics access. If a program takes away the basic tools needed to manage limited work responsibilities, many executives won't enter care.

What functional luxury actually means
Executive treatment should be designed around continuity, not theater. Programs in this category are built to support work obligations through private rooms for all residents and dedicated business centers with cellphone and internet access, as described in this overview of executive treatment accommodations.
That model matters because executives often need to do some of the following while in care:
- Review sensitive communications: Limited email and phone access can prevent unnecessary panic at work.
- Attend a critical meeting: Some responsibilities can't disappear overnight, especially for owners and C-suite leaders.
- Protect professional identity: Private rooms reduce exposure and support discreet scheduling.
- Preserve cognitive bandwidth: Quiet office-like spaces help clients complete essential tasks without derailing treatment hours.
What to insist on before admission
A serious professional should ask for clarity on logistics, not vague reassurances. The right questions are practical.
- Electronics policy: Are phones and laptops permitted, and under what clinical boundaries?
- Private accommodations: Does every resident have a private room in detox and residential treatment?
- Work scheduling: Can the program coordinate limited access around therapy rather than force an all-or-nothing choice?
- Confidential communication: How are sensitive calls, legal matters, or board-level obligations handled?
For professionals managing neurodivergence alongside stress, anxiety, or burnout, workplace support planning also matters after discharge. This guide on support for ADHD and autism at work is a useful resource when discussing accommodations and sustainable re-entry with employers.
Career continuity should be structured, not unlimited
Good executive care does not mean unrestricted work. That defeats the purpose. It means bounded access that preserves treatment as the priority while allowing essential obligations to be managed intelligently. Programs that handle this well usually create a specific plan for call windows, laptop use, meeting exceptions, and communication with assistants or family office staff. A practical example of that model appears in this discussion of how to work from rehab.
Privacy and work access only help when clinical boundaries remain intact. The point is controlled continuity, not bringing the entire office into treatment.
Expensive private-pay care earns its price. It removes friction. It gives the client the conditions needed to commit fully enough to treatment without setting off avoidable professional fallout.
Admissions Length of Stay and Aftercare Planning
Busy professionals often delay residential mental health treatment because they assume admissions will be chaotic, public, or drawn out. A well-run private-pay program should be the opposite. It should move quickly, communicate clearly, and protect confidentiality at every step.
The sequence is usually straightforward. Clinical screening comes first, followed by review of mental health symptoms, substance use, medications, work constraints, and any immediate detox needs. From there, the program can determine fit, timing, and the right structure for arrival.
How long treatment usually lasts
Executive-focused residential care is rarely a weekend fix. The typical length of stay at a private luxury rehab with executive programming ranges from 30 to 90 days, as described in this overview of luxury executive rehab options.
That range makes sense. Early days are often spent stabilizing sleep, mood, anxiety, cravings, and cognitive overload. Once the client is no longer operating in constant threat mode, deeper therapy becomes more productive. Time is what allows the treatment team to identify patterns, test new coping strategies, and build a discharge plan that isn't aspirational nonsense.
Cost should be viewed like any other major risk decision
For elite private-pay care, the financial commitment is substantial. A 30-day stay in a high-end executive treatment program typically ranges from $80,000 to $150,000, reflecting the confidential, individualized, and clinically intensive nature of this level of care, according to this guide on executive rehab pricing.
That price point is not for everyone. But for executives making high-stakes decisions every day, the better lens is risk management.
- Untreated instability can damage leadership judgment, relationships, legal standing, and long-term earning power.
- Inadequate treatment often leads to repeat episodes, public fallout, or expensive disruption later.
- Comprehensive care gives a client a chance to resolve the actual problem rather than repeatedly contain its consequences.
Aftercare is where serious programs prove themselves
Discharge is not the finish line. It is a transition point.
Strong aftercare planning should include ongoing therapy, psychiatric follow-up when indicated, recovery support, family work when appropriate, alumni programming, and clear guidance on returning to work, travel, and social events. The point is continuity. Without it, even a strong residential stay can lose traction under real-world pressure.
A professional should never choose a program based only on admissions speed or property aesthetics. The more important question is whether the team already thinks several months ahead.
Frequently Asked Questions About Executive Treatment
Is privacy actually protected
It should be, and any serious executive program treats confidentiality as a core operational issue. That includes discreet admissions, protected communication, private accommodations, and careful handling of who knows what. If a program is vague about privacy, it isn't the right fit for a high-profile client.
Can family be involved without taking over the process
Yes. In fact, selective family involvement often improves outcomes when it is clinically guided. The key is control. Some clients need spouses or relatives included early. Others need a measured pace while trust and stability are rebuilt.
Can a client keep working during treatment
In executive-focused care, limited work continuity is often possible. The right model allows essential responsibilities to be managed within boundaries. Treatment must remain primary, but career obligations don't have to disappear completely for care to work.
What if travel or a major meeting comes up
That should be addressed before admission, not improvised in the middle of treatment. Some issues can be managed through scheduling, remote communication, or delegation. If a client already knows there are immovable obligations, the clinical team should build around them carefully rather than pretend they don't exist.
Is private pay the only option
For many luxury executive programs, yes. Some clients may still pursue out-of-network reimbursement depending on their benefits and documentation, but the primary financial structure is usually private pay. A competent admissions team should explain that plainly and help organize paperwork where appropriate.
How does a client know a program is clinically serious
The fastest test is direct questioning. Ask about accreditation, psychiatric coverage, dual diagnosis capability, detox oversight, individualized treatment planning, family work, electronics policy, and aftercare design. A strong program answers directly. A weak one hides behind polished language.
Reflections offers private-pay, Joint Commission-accredited residential care for adults who need discreet dual-diagnosis treatment in a private setting, with private rooms, electronics access, clinically managed detox when appropriate, and continuing care built for long-term recovery. Executives, professionals, and families who want a confidential discussion of fit, timing, and treatment options can learn more through Reflections.