A senior leader can manage litigation, investor pressure, and organizational change with composure, then feel blindsided by a spouse's guarded tone, an adult child's distance, or the politics of a company dinner where everyone expects a drink in hand. That isn't hypocrisy. It's a fact that relationships during recovery involve a different kind of risk exposure than most professionals are trained to manage.
In executive life, people often treat personal dynamics as background noise until they become operational threats. Recovery changes that calculus. The people closest to a person can either stabilize the work of treatment or destabilize it through conflict, secrecy, resentment, or misplaced loyalty. For high-performing professionals, the stakes are wider than emotional discomfort. Reputation, leadership credibility, family systems, succession planning, and career continuity can all be affected by how relationships are handled in the months after treatment begins.
This is one reason the recovery literature matters so much here. Roughly 22.3 million Americans, more than 9% of U.S. adults, live in recovery, and social support is repeatedly identified as a major protective factor. The same source notes that 70% of people who receive treatment report better quality of life and functioning within one year, reinforcing that relationship stability and family involvement are part of a successful recovery environment, not peripheral concerns, according to healthy relationships in recovery research.
The New Bottom Line Navigating Relationships in Recovery
For executives, recovery works best when it's treated as a full-spectrum stability plan. That includes clinical care, daily routines, sleep, medical oversight, and the human environment surrounding all of it. A board can survive one bad quarter. Recovery is less forgiving when the home environment stays chaotic or when one key relationship becomes the sole source of emotional regulation.
The mistake many accomplished professionals make is assuming that intelligence and discipline will solve relationship strain quickly. They usually won't. Loved ones may still be angry after treatment starts. Colleagues may misread new limits as withdrawal. A spouse may want transparency that feels invasive. None of that means treatment isn't working. It means recovery is exposing systems that were previously held together by crisis management.
What executives often get wrong
Three patterns tend to create avoidable problems:
- Using performance logic in intimate settings: Efficiency matters at work. At home, trust rebuilds through repeated, ordinary reliability.
- Expecting gratitude too early: Family members may feel relief, skepticism, grief, and anger at the same time.
- Overconcentrating support in one person: When a spouse, partner, or close friend becomes the entire support structure, any conflict can threaten sobriety.
Practical rule: If a relationship creates secrecy, emotional volatility, or pressure to manage someone else's distress at the expense of recovery tasks, it deserves the same level of scrutiny as any other relapse risk.
What works instead
A more durable approach is to treat relationship management as a governance issue. That means asking clear questions. Which relationships are stabilizing? Which ones are draining? Where does accountability live? Who gets what information, and when? What contact patterns support treatment rather than compete with it?
For high-achieving clients, this reframing is often a relief. It replaces vague advice like “work on your relationships” with a sharper mandate. Build a recovery environment where trust can be earned, limits can be enforced, and important relationships can develop on the basis of reality rather than damage control.
How Recovery Reshapes Your Closest Relationships
Recovery rarely changes just one person. It changes the operating system of the household. In many families, addiction creates informal roles that feel stable even when they're unhealthy. One person overfunctions. Another minimizes. Someone becomes the peacemaker. Someone else tracks moods, covers absences, or manages fallout. Once recovery begins, those roles stop working the way they used to.
That's why relationship strain in early treatment shouldn't automatically be read as failure. It often reflects restructuring. A family that adapted around crisis now has to adapt around honesty, uncertainty, and new expectations.
The corporate restructuring analogy
Executives usually understand this quickly when it's framed the right way. Think of recovery as a corporate restructuring after a long period of poor controls. The old system may have produced revenue, but it also hid liabilities, encouraged workarounds, and rewarded short-term patches over durable performance. Recovery introduces new controls. Suddenly, the former “fixes” are identified as part of the problem.
In relationships, that can look like this:
- Old communication scripts break down: People can't rely on avoidance, half-truths, or reassurance on demand.
- Decision rights shift: The person in recovery may need firmer limits around schedule, social events, or travel.
- Emotional reactions intensify before they settle: Family members may test whether change is real.
A visual model helps clarify the pattern:
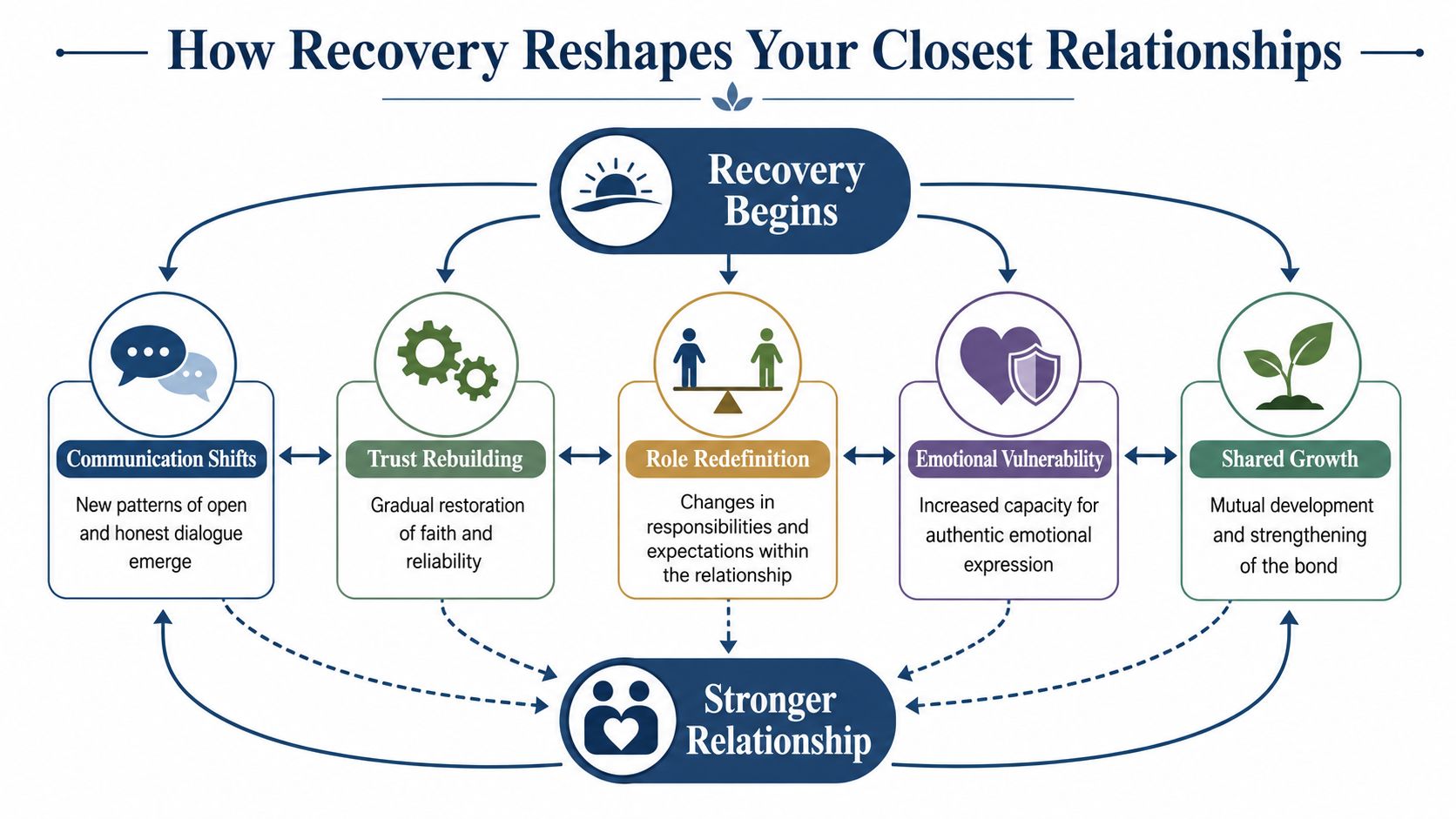
The system has to relearn trust
Many clients want their family to “move forward.” Families usually want evidence before they do. That evidence doesn't come from one conversation. It comes from a new pattern of behavior that everyone can observe over time.
This is also where outside support can be useful. Families often need structure of their own, not just updates on the patient's progress. Thoughtful, evidence-informed family guidance can help loved ones respond without slipping back into old roles of rescuing, monitoring, or escalating.
Recovery often improves relationships by making hidden patterns visible. The discomfort comes first. The clarity comes after.
Why this matters clinically
The larger point is practical. Relationship quality affects recovery conditions. Supportive ties help create accountability, reduce isolation, and make honesty more sustainable. Negative ties do the opposite. They pull attention away from treatment tasks and back into instability.
For professionals who remain engaged with work while receiving care, this matters even more. If a client is balancing treatment with active leadership responsibilities, the family system can't be left unmanaged. The emotional climate at home becomes part of the recovery plan, just as much as therapy, medication review, and relapse prevention.
Rebuilding Trust with Family and Spouses
Trust doesn't come back because someone finally says all the right things. It comes back when other people stop having to guess what kind of day they're walking into. That distinction matters. In families affected by addiction, apologies are often plentiful long before consistency appears.
For spouses and relatives, trust is less about forgiveness than predictability. They want to know whether commitments will be kept, whether money is being handled with integrity, whether mood changes will be acknowledged rather than denied, and whether difficult conversations can happen without intimidation or collapse.
The mechanics of repair
A practical repair process usually includes several moves happening at once:
- Narrow the promise set. Small commitments kept repeatedly matter more than broad vows.
- Increase verifiability. Calendars, schedules, financial clarity, and agreed check-ins reduce ambiguity.
- Accept delayed confidence. Loved ones may need a long proof period before they soften.
- Stop asking for premature emotional closure. “Can't we move on?” is usually heard as “Stop having a memory.”
A useful way to frame this for executives is credit restoration. When trust has been overdrawn, the account isn't repaired by one large deposit. It's repaired by a long run of accurate, uneventful payments.
| Trust builder | What it looks like |
|---|---|
| Reliability | Arriving on time, following through, staying reachable within agreed limits |
| Transparency | Answering reasonable questions without defensiveness or selective disclosure |
| Emotional regulation | Staying present in hard conversations instead of retreating, attacking, or manipulating |
| Respect for impact | Letting loved ones name harm without arguing over every detail |
When repair isn't the right goal
Not every relationship should be restored. That can be hard for successful professionals to accept because they are used to solving complex problems with enough effort and expertise. Some relationships aren't repair projects. They are chronic threat environments.
Recovery guidance has to make room for that reality. Guidance on navigating relationships during recovery notes that not all intimate relationships are salvageable and emphasizes the need to identify patterns of vulnerability while asserting personal and child safety at all times.
Some families need reconciliation. Others need distance, documentation, and a safety plan.
When betrayal has been part of the relationship story, practical resources on handling relationship doubts and betrayal can help partners think more clearly about what rebuilding should require, and what warning signs should stop the process.
For couples who do have a viable foundation, structured therapeutic work often matters more than private promises. Programs that include couples and family sessions for healing relationships can provide a contained setting to address disclosure, resentment, finances, and boundaries without letting every discussion turn into an unmoderated replay of old injuries.
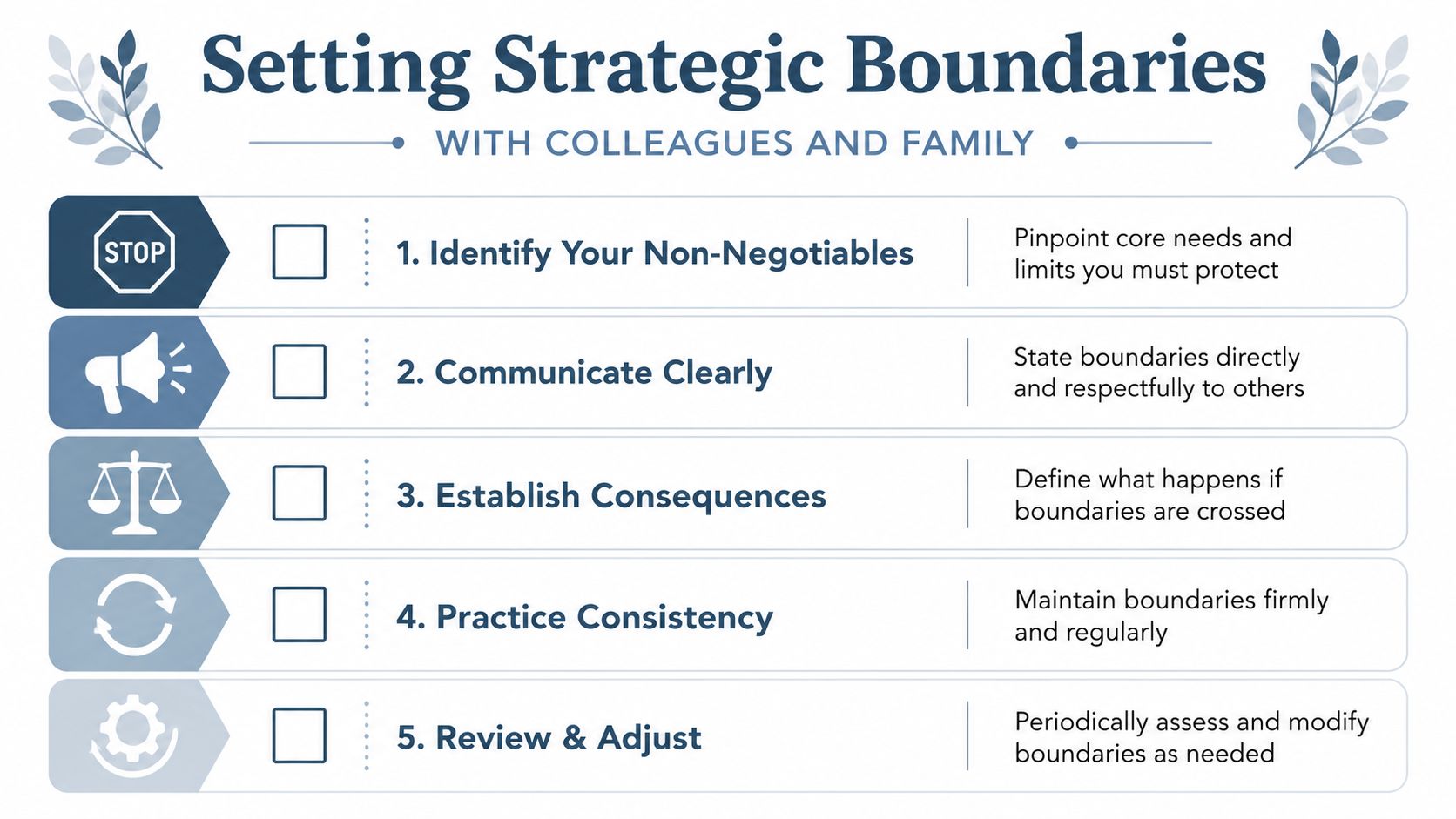
Setting Strategic Boundaries with Colleagues and Family
Many professionals hear the word “boundary” and assume it means distance, coldness, or conflict. In reality, boundaries are operating protocols. They tell people how access will work, what topics are open, what settings are unsafe, and what happens when a limit is ignored. In relationships during recovery, that level of clarity isn't rigid. It's protective.
Qualitative evidence in stable substance use disorder recovery found that positive intimate relationships support long-term abstinence when they reduce shame and reinforce self-agency. The same work found that people often had to actively protect themselves from negative relationships, which makes boundary-setting a clinical skill for relapse prevention, not a personality preference, according to qualitative research on recovery relationships.
Boundaries at work
Executives usually need boundaries that are brief, professional, and hard to misinterpret.
- For alcohol-centered events: “I'm attending for the business purpose, leaving early, and not staying for the after-hours portion.”
- For intrusive questions: “That's personal, but performance and availability are fully covered.”
- For after-hours contact: “Nonurgent matters can wait until morning. Urgent issues should come through the agreed channel.”
These aren't emotional speeches. They're clear instructions.
People who struggle to hold that line often benefit from practical models used in leadership coaching and wellness settings. Resources on expert strategies to manage work-life balance can help professionals translate personal limits into language that still fits a high-accountability role.
Boundaries at home
Family boundaries need a different tone. They can be warmer, but they still need structure.
Common examples include:
- Topic limits: “This isn't a good time to revisit past incidents. That conversation belongs in therapy.”
- Access limits: “Unannounced visits won't work right now.”
- Event limits: “If substances are central to the gathering, attendance may not be appropriate.”
- Rescue limits: “Covering consequences or making excuses won't be part of this process.”
What boundary failure looks like
Boundary failure rarely starts with one dramatic collapse. It usually starts with small exceptions made for convenience, guilt, image management, or conflict avoidance. A leader agrees to one dinner that feels unsafe. A spouse asks for all-day reassurance and gets it. A sibling demands details that were never theirs to have. The pattern expands.
That's why consistency matters more than eloquence. A simple boundary repeated calmly is stronger than an impressive one enforced once. For clients dealing with chronic people-pleasing, approval-seeking, or overfunctioning in close relationships, targeted treatment such as codependency-focused support may be clinically relevant because it addresses the relational habits that often undermine recovery long after detox is over.
The One Year Rule and Modern Dating for Professionals
The question comes up constantly. When is it safe to start dating again?
The most common clinical answer is conservative for a reason. A broad relapse-prevention consensus recommends waiting at least one year into recovery before starting a new relationship, and multiple treatment sources echo that benchmark in guidance on new relationships after recovery. The point isn't moral caution. It's stabilization.
Why the timing matters
New romance introduces volatility even when it's healthy. There's anticipation, uncertainty, projection, sexual chemistry, disappointment, negotiation, and the pressure to be chosen. In early recovery, those states can compete directly with treatment work.
For professionals, there's another layer. Dating often happens in environments that reward image, speed, and novelty. That can mean business dinners, travel, networking overlap, private messaging late at night, and social scenes where substances are normal. A person may believe they are evaluating a potential partner when, in reality, they are also stress-testing their own regulation.
A new relationship can feel supportive and still be badly timed.
A practical screening lens
Instead of asking only, “Do they like me?” a better set of questions is:
- Does this relationship increase or decrease pressure?
- Is there room for honesty about recovery without performance?
- Does the person use substances in ways that would destabilize the environment?
- If this ends abruptly, is sobriety protected by other support structures?
For some professionals, the answer may still be no dating for now. For others, the answer may be limited, highly intentional social contact rather than rapid attachment. The benchmark should be emotional steadiness, established support outside the relationship, and a demonstrated ability to tolerate loneliness without acting impulsively.
This is one area where status can be misleading. Sophistication, success, and social fluency don't reduce romantic risk in early recovery. They often increase access to high-intensity situations and make it easier to rationalize them.
When to Disclose Your Recovery in the Workplace
Workplace disclosure is not a character test. It's a strategic decision. Some professionals benefit from selective transparency. Others protect recovery better by keeping information tightly held. The right choice depends on role, company culture, legal considerations, reporting lines, and how much practical support disclosure would create.
The same logic used in intimate relationships applies here. Timing and trust matter. A supportive colleague can be helpful. The wrong disclosure to the wrong person can create gossip, stigma, or unnecessary vulnerability. Guidance on intimacy and recovery notes that who a person trusts, and when, is a central risk-management decision because support can help while poorly timed stressors can destabilize recovery.
A side-by-side decision frame
| Option | Potential upside | Potential downside |
|---|---|---|
| Tell no one beyond immediate necessity | Maximum privacy, tighter reputation control | Less support, fewer accommodations, more solo management |
| Tell HR or a designated executive contact | Clearer documentation, possible workplace protections, structured planning | Permanent record within the organization, trust required |
| Tell a direct supervisor only | Operational alignment, easier scheduling conversations | Outcome depends heavily on manager maturity and discretion |
| Tell selected peers | Day-to-day support and fewer awkward social assumptions | Higher risk of drift, oversharing, or informal spread |
Practical disclosure questions
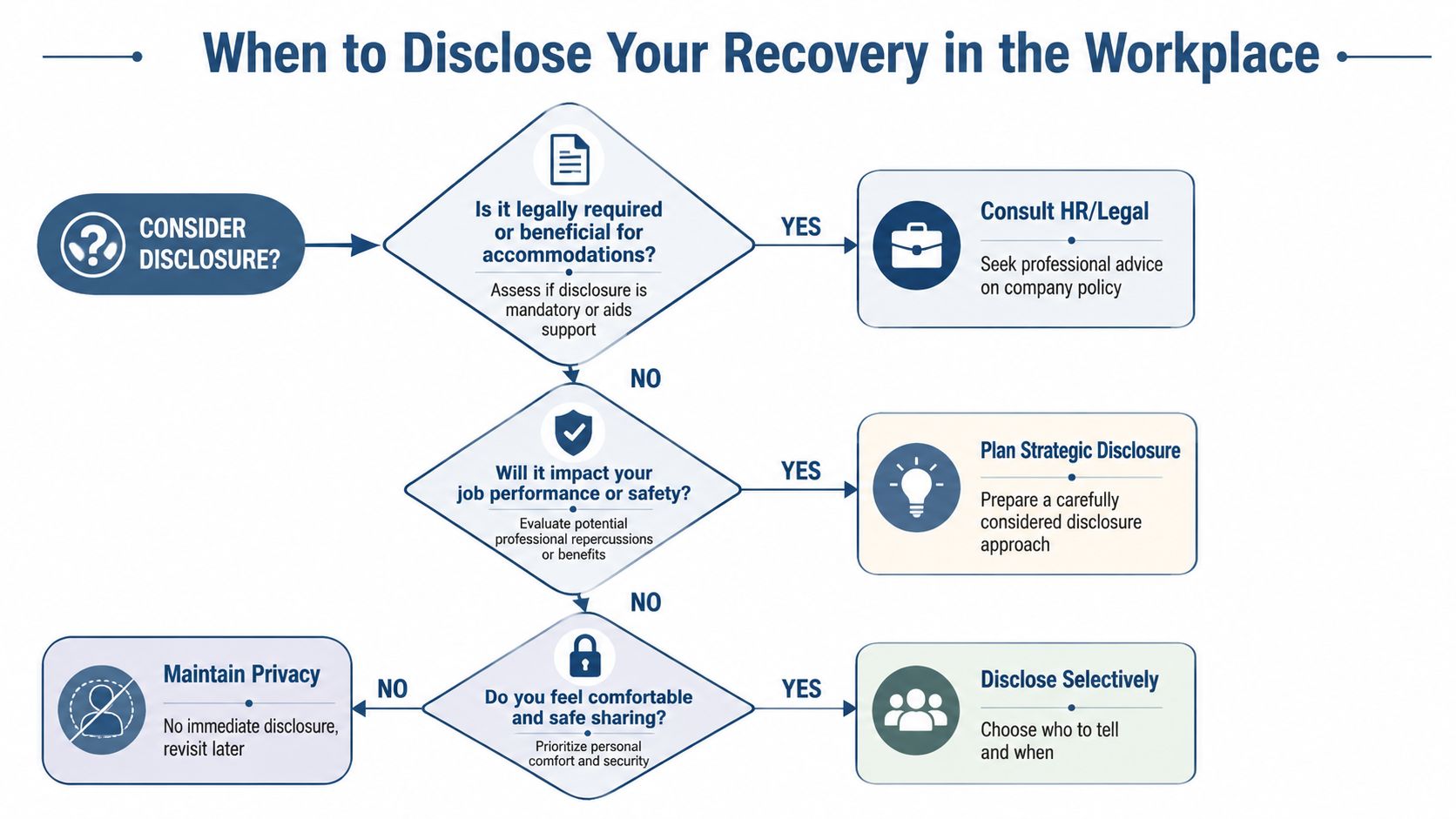
Before saying anything, a professional should assess:
- Is disclosure necessary for accommodations or leave coordination?
- Will recovery-related scheduling affect performance visibility?
- Has this person handled confidential information well in the past?
- What is the minimum information needed to achieve the objective?
This visual can help organize the decision:
What selective disclosure sounds like
Most disclosures should be short and purpose-driven. “A health matter required treatment, care is in place, and work continuity is being managed” is often enough. Not every workplace contact needs the full history. In fact, selective disclosure is usually the more disciplined approach.
For professionals preparing for that conversation, guidance on talking to an employer about rehab can help clarify what to say, what not to say, and how to protect both recovery and career standing.
Your Continuing Care Plan for Relationships
Relationship health shouldn't be treated as a one-time repair project completed at discharge. It functions more like continuing care. The underlying question is not whether conflict will ever return. It's whether the person now has systems strong enough to respond without sliding back into secrecy, avoidance, or chaos.
That means reviewing relationship risk the same way a serious professional reviews any other exposure. Which ties are restorative? Which settings are still unreliable? Where are the old vulnerabilities most likely to reappear? Family friction, social pressure, and loneliness don't disappear because treatment was effective. They become manageable when they are anticipated.
What ongoing maintenance looks like
A sound relationship plan often includes:
- Scheduled family or couples work: Not only crisis sessions.
- Clear communication agreements: Especially around travel, social events, and financial stress.
- Support redundancy: No single person carries the entire emotional load.
- Periodic boundary review: Limits may need tightening or relaxing as recovery matures.

For high-earning professionals, the practical standard is straightforward. Relationships should support sustained recovery, not consume it. A private, clinically sophisticated setting can help establish that standard by combining dual-diagnosis treatment, family involvement, continuing care, and work-compatible structure. At Reflections, that may include private family sessions, monthly educational workshops, ongoing therapeutic support, and treatment planning that accounts for the realities of leadership, confidentiality, and continued access to work responsibilities.
The objective isn't a perfect family system or a frictionless marriage. It's a more stable life, built around honest relationships that can hold pressure without collapsing under it.
Relationship strategy deserves the same seriousness as any other part of recovery planning. For professionals who need confidential, clinically rigorous care that also respects career obligations, Reflections provides private, upscale dual-diagnosis treatment with appropriate access to electronics, private rooms, family involvement, and continuing support designed for long-term stability.