
A senior executive often reaches treatment at the same point. Performance still looks intact from the outside, but sleep is poor, alcohol or medication use has become private and habitual, anxiety is harder to contain, and home life is carrying the strain. The usual advice, “step away from everything and check into a standard program,” doesn't fit the circumstances of board obligations, sensitive communications, public visibility, or the simple fact that a high-functioning life is still in motion.
That's where personalized treatment planning matters. For professionals with complex schedules, significant responsibilities, and co-occurring mental health and substance use issues, treatment has to do more than remove substances and provide therapy. It has to organize care around privacy, medical safety, psychological depth, family realities, and the demands of a life that cannot be casually paused.
Beyond One-Size-Fits-All Recovery
A generic program often assumes that every client can follow the same schedule, tolerate the same group intensity, respond to the same therapeutic pacing, and disconnect from work in the same way. Executives and other high-performing professionals rarely fit that template.
Some arrive with alcohol dependence and severe insomnia. Others are managing stimulant misuse, panic symptoms, depression, trauma, or a cycle of overwork followed by collapse. Many have spent years using competence as camouflage. They don't need a more polished version of standard rehab. They need a plan that understands complexity from day one.
A luxury setting matters here, but not for appearances. It matters because privacy, quiet, private rooms, and clinical access change what can be addressed openly. A person who feels exposed or treated like a stereotype will protect image instead of engaging in treatment. A person who feels respected is far more likely to tell the truth about sleep, substances, relationships, shame, and the pressures tied to leadership.
Daily regulation also matters more than many families realize. For professionals whose stress systems have been running hot for years, sleep disruption is often both a symptom and a driver of relapse risk. Resources like SleepHabits' wellness insights can help families understand why recovery has to include restoration, not just abstinence.
For clients looking for care that aligns with a demanding life, discreet personalized treatment that fits a professional lifestyle is a more realistic framework than the old all-or-nothing model.
A strong treatment plan doesn't ask a professional to become someone else. It helps that person recover without abandoning the responsibilities, identity, and standards that matter to them.
What Personalized Treatment Planning Truly Means
A real personalized treatment plan isn't just “individual therapy plus a few preferences.” It's a structured clinical process that asks a harder question: given this person's psychiatric profile, substance use pattern, stress load, medical status, professional responsibilities, family system, and history of coping, what treatment mix is most likely to work now?
That's the difference between an off-the-rack suit and a bespoke one. Both cover the body. Only one is built around the person wearing it.

It's dynamic, not decorative
In practice, personalized treatment planning changes the sequence, intensity, and coordination of care. A client with trauma and alcohol dependence may need early nervous-system stabilization before deeper trauma processing. A client with bipolar features, insomnia, and overuse of prescribed medication may need careful psychiatric review and pacing before being placed into emotionally demanding work.
That's why personalization isn't a branding term. It's clinical architecture.
Machine-learning driven planning is most useful when it models heterogeneous treatment effects, meaning it helps estimate which intervention is more likely to benefit a specific patient based on variables such as history, severity, comorbidity, and behavior, rather than predicting general risk, as described in this discussion of individualized response modeling.
What it includes in luxury executive care
For high-functioning clients, a plan usually has to account for more than diagnosis. It often includes:
- Professional stress exposure: decision fatigue, public pressure, travel rhythms, and constant availability
- Confidentiality needs: who can know, what can be shared, and how communication is handled
- Functional obligations: whether limited electronics access supports stability or destabilizes it
- Relationship realities: spouse strain, family distrust, or workplace enabling
- Treatment tolerance: some clients can move quickly into insight work, others first need sleep, detox support, and cognitive recovery
A personalized plan should also clarify what success looks like. For one executive, success may mean safe detoxification and mood stabilization. For another, it may mean learning to stop using work intensity to outrun grief, depression, or panic.
Clients who want a more detailed view of this model can review customized mental health and addiction treatment, where individualized planning is treated as a core clinical method rather than a surface-level amenity.
The Clinical Architecture of a Bespoke Plan
The strongest personalized treatment planning has structure. Without structure, “individualized care” becomes improvisation. High-end clinical work should feel precise, coordinated, and accountable.
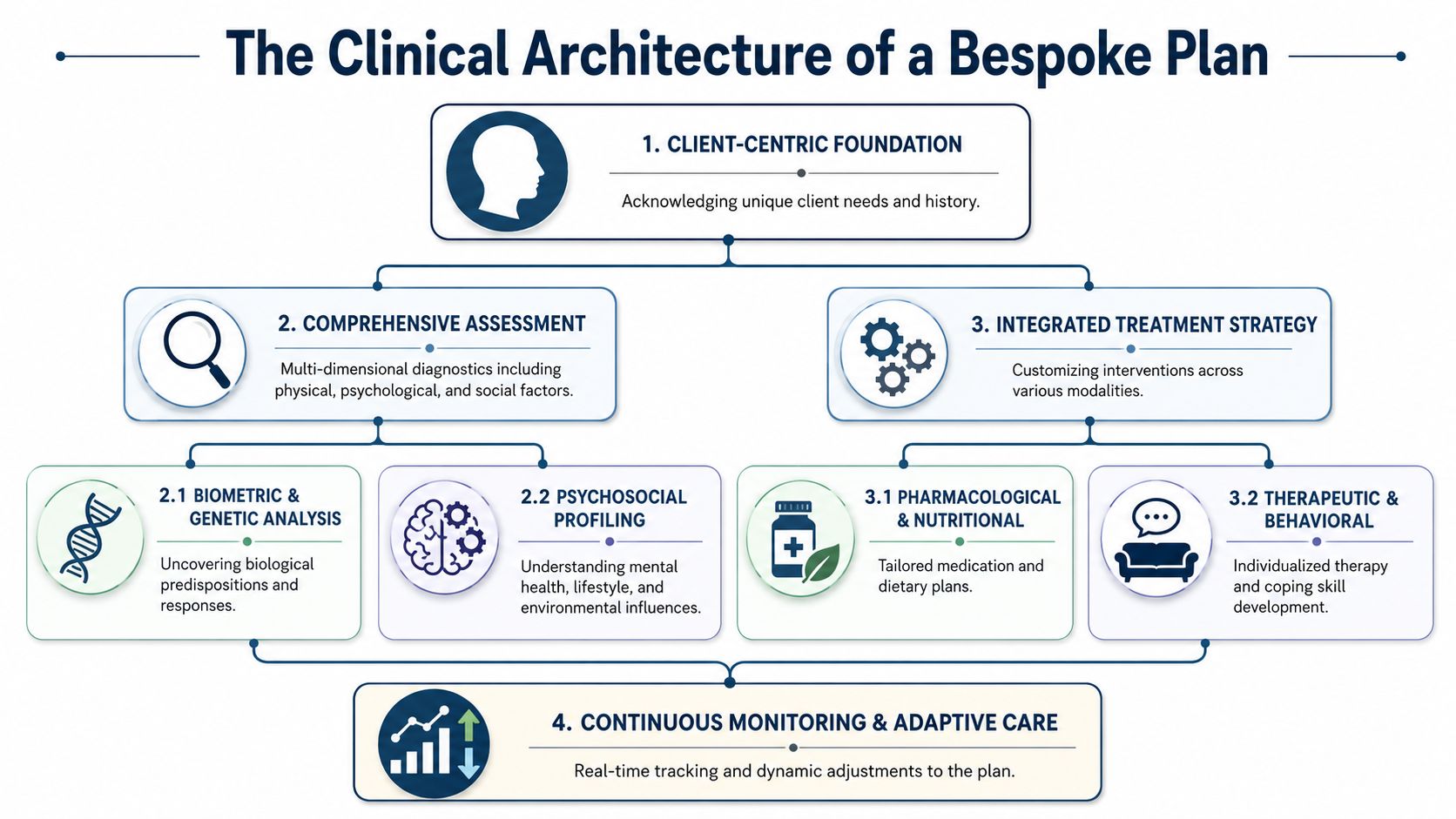
Assessment that goes beyond intake
A real assessment does more than gather symptoms. It builds a working model of how the person functions under stress, what substances or behaviors serve psychologically, what co-occurring conditions are active, and where immediate risks sit.
For professionals, this usually means examining several layers at once:
- Medical status: withdrawal risk, sleep disruption, medication interactions, pain issues, and physical depletion
- Psychiatric picture: anxiety, depression, trauma, obsessive traits, mood instability, or executive burnout
- Behavioral pattern: secrecy, overcontrol, emotional avoidance, perfectionism, or reward-seeking
- Context: marriage, parenting, legal concerns, reputation management, and work demands
The same outward problem can have very different clinical drivers. For example, two executives may both drink nightly. One is self-medicating unresolved trauma. The other is blunting hypomanic agitation and chronic insomnia. Treatment should not pretend those are identical cases.
Shared goals that are clinically useful
Collaborative goal-setting isn't a soft concept. It's a measurable workflow. In a Veterans Health Administration personalized health planning program, 91.7% of patients reported that they explored what they wanted for their health and set shared goals, and 97.2% said the experience was better than a traditional office visit, according to the published program findings.
That result matters because treatment adherence improves when the plan reflects the client's own priorities. For an executive, those priorities may include restoring sleep, stabilizing mood before a board return, repairing credibility at home, reducing medication burden, or learning how to work without relying on alcohol at night.
Practical rule: If a client can't explain the goals of treatment in plain language, the plan isn't clear enough yet.
The process is similar to bespoke travel design. Travelers often prefer personalized luxury tours because the itinerary reflects pace, interest, and context instead of forcing everyone through the same route. Clinical planning works the same way, except the stakes are far higher.
Curating the treatment mix
Once the assessment is clear, the team selects modalities for function, not fashion. That can include individual psychotherapy, psychiatric management, skills-based work, family sessions, trauma-informed care, mindfulness, somatic work, fitness, nutrition support, and carefully structured group participation.
Not every client needs every modality at the same intensity.
A useful way to think about selection is below:
| Clinical need | Common planning response |
|---|---|
| Acute emotional volatility | More stabilization, closer psychiatric review, slower trauma pacing |
| Cognitive overload and exhaustion | More sleep restoration, reduced stimulation, concrete skill work |
| Family distrust | Earlier family sessions, expectation-setting, accountability work |
| Work-related pressure | Structured communication windows, boundaries coaching, relapse mapping around performance stress |
Medication planning also deserves scrutiny. In executive populations, overmedication can blunt engagement, while undertreatment can leave destabilizing symptoms untouched. The right approach is often minimal, precise pharmacology with ongoing review. That's one reason many families look closely at the role of on-site medical directors in luxury dual-diagnosis treatment, especially when detox, psychiatric symptoms, and professional functioning all intersect.
A Sample Executive Treatment Pathway
A personalized plan shouldn't feel vague. It should translate into a lived treatment pathway that adapts as the client stabilizes. For an executive or business owner, that pathway often has phases rather than a fixed script.
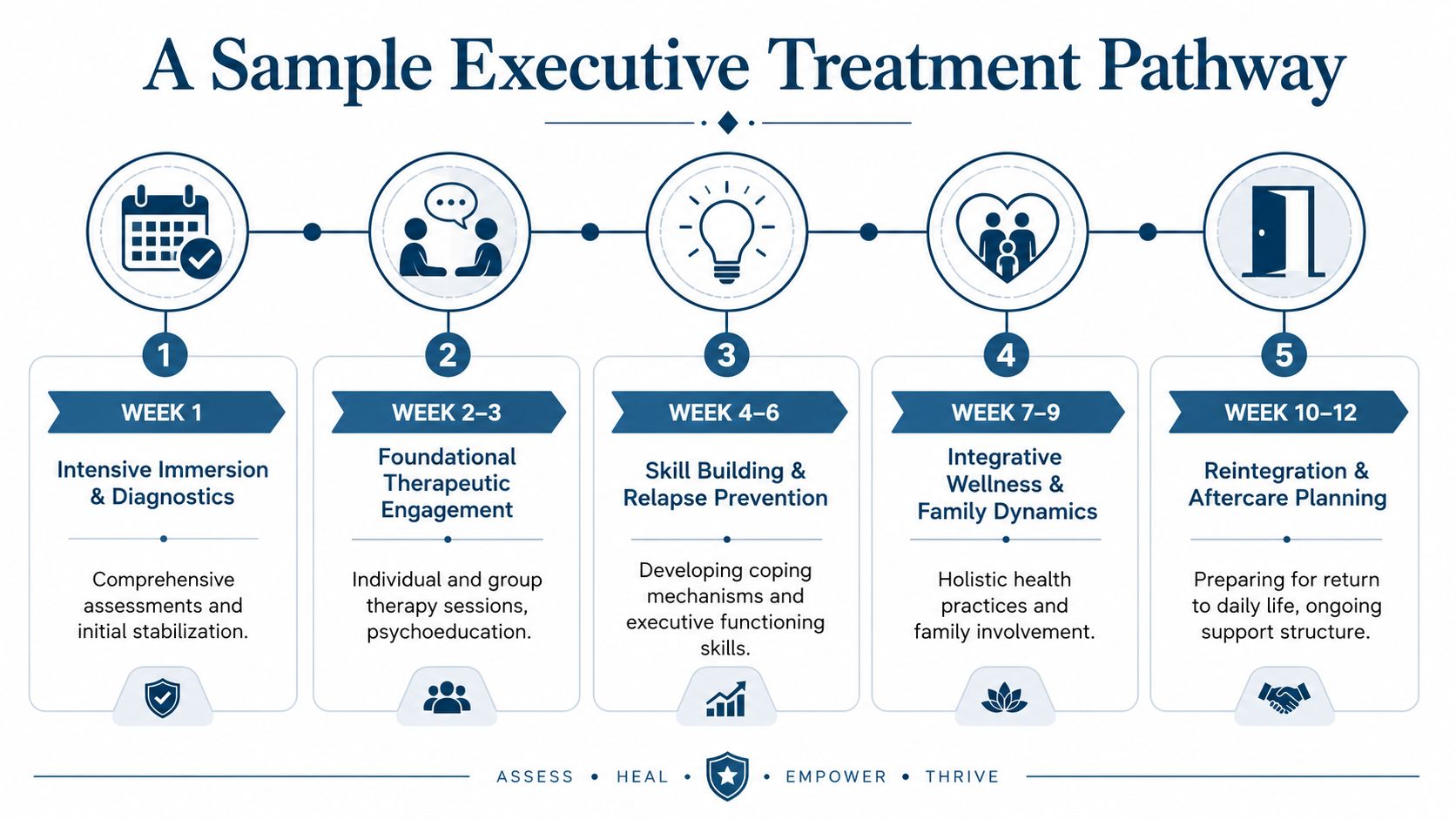
Early phase
In the opening stretch, the priorities are medical safety, psychiatric clarity, and nervous-system stabilization. If detox is needed, it should happen in a private setting with close observation and a clear medication strategy. Sleep is often addressed immediately, because poor sleep can distort mood, impulse control, and treatment engagement.
Electronics access may be limited but not eliminated. For some professionals, a short, structured window for urgent communication lowers panic and resistance. For others, constant device access keeps the stress cycle fully active and interferes with treatment from the first day. The plan should distinguish between real responsibility and compulsive attachment.
Middle phase
Once the client is medically steadier, the work becomes deeper. At this stage, therapy starts linking substance use to pressure, identity, trauma, grief, perfectionism, or emotional isolation. A professional who has spent years solving other people's problems may need to learn basic internal skills that were never built under stress.
The weekly rhythm might include:
- Individual psychotherapy: to identify root causes, distorted beliefs, and relapse drivers
- Skills work: emotional regulation, communication, boundaries, and stress recovery
- Psychiatric review: to assess response, side effects, and whether symptoms are changing
- Family or partner sessions: to address secrecy, resentment, and realistic expectations
- Protected work blocks: used selectively and clinically, not as an open invitation to remain fully on duty
Recovery for a high-performing client often depends on teaching selective engagement. The goal isn't constant availability. The goal is stable functioning.
Reintegration phase
Later treatment shifts toward re-entry. That doesn't mean discharge planning is reduced to a list of appointments. It means the team pressure-tests the plan against real life.
Questions become more specific. What happens at the first business dinner where alcohol is present? How will the client respond to insomnia after travel? What does a spouse need to see before trust begins to return? Which relationships support stability, and which ones normalize overwork and self-neglect?
A sound pathway should produce a continuing-care structure that matches the client's life after residential care, including psychiatric follow-up, therapy cadence, recovery support, family work, and practical boundaries around devices, travel, and work intensity.
The Reflections Difference in Personalized Care
A senior executive arrives willing to do treatment, but not willing to disappear from a company, a family, and a public-facing role overnight. That client does not need a prettier setting. That client needs a clinical environment built for privacy, honest assessment, and disciplined flexibility.
Luxury matters only when it improves care. Personalized treatment planning breaks down when the setting looks polished but the clinical work is generic, fragmented, or too rigid for the life the client is returning to.
For professionals with dual-diagnosis needs, a private-pay residential setting gives the team more control over pace, privacy, and clinical focus. That changes the work in practical ways. Psychiatric symptoms, substance use, medication response, family strain, and work-related pressure can be evaluated together instead of in separate silos. Private rooms support that process because clients sleep better, regulate faster, and have space to think between demanding sessions.
Why environment changes clinical quality
High-functioning clients often know how to look stable while remaining unwell. In a busy or socially exposed setting, that performance can continue for weeks. In a more private residential environment, with fewer distractions and more discretion, the presentation often becomes more accurate. Assessment improves. Therapy gets more honest. Treatment decisions get better.
Electronics access is part of that judgment. It is not a courtesy item for this population. It is a clinical variable.
Some clients benefit from structured, time-limited contact with work so treatment remains realistic and credible. Others use work contact to avoid grief, anxiety, withdrawal, shame, or family repair. A strong program can tell the difference and set limits accordingly, rather than treating all device access as either harmless or forbidden.
Real personalization requires ongoing review
A personalized plan should keep changing as the client changes. Symptom patterns, sleep, engagement in therapy, family feedback, and functional capacity need regular review so the team can adjust treatment based on current presentation, not intake assumptions. Research on precision approaches in mental health supports repeated measurement and adaptation rather than static planning, as explained in this review of precision approaches in mental health.
In an executive-focused setting, that review helps answer the questions that matter most:
- Is the client stabilizing, or only presenting well?
- Is therapy producing usable change, or just polished insight?
- Are professional responsibilities being managed appropriately, or feeding the same stress cycle?
- Is the medication strategy improving judgment, sleep, and emotional range, or just flattening distress?
Reflections is a California-licensed, Joint Commission-accredited luxury dual-diagnosis residential provider offering private rooms, clinically managed detox, individualized treatment planning, and appropriate electronics access for adults balancing recovery with ongoing professional responsibilities.
Personalized care is defined by clinical judgment. The right team keeps adjusting the right variables at the right time.
Measuring Success Beyond Sobriety
Sobriety matters. It's just not the whole picture.
A high-achieving client can stop using substances and still return home emotionally unavailable, cognitively depleted, sleep-disrupted, rigid under pressure, and prone to relapse the moment professional demands intensify. That's not durable recovery. That's temporary interruption.

What families and professionals should actually watch
In executive treatment, better markers of progress often include:
- Clearer judgment: less impulsive decision-making, better prioritization, more realistic self-appraisal
- Emotional range: the ability to feel stress, disappointment, or conflict without immediately numbing
- Relational repair: more honesty, more consistency, fewer defensive reversals
- Functional stability: improved sleep, steadier energy, and healthier use of time
- Pressure tolerance: staying grounded during difficult calls, deadlines, travel, and interpersonal strain
These are the outcomes that make abstinence sustainable.
Why rigor matters
There's also an important caution here. Personalized treatment planning sounds intuitively superior, but intuition isn't enough. Analysis of clinical trial data shows that creating personalized rules does not automatically produce better outcomes, and some constructed rules performed worse than standard treatment, which is why rigorous validation is essential before relying on a tailored model.
That has direct implications for families choosing care. A premium program shouldn't only promise customization. It should show disciplined clinical reasoning, integrated review, and the ability to change course when an initial plan isn't working.
The standard for success shouldn't be “the client completed treatment.” It should be whether the client returns to life with more capacity, more honesty, and a recovery structure strong enough to hold under real-world pressure.
Frequently Asked Questions About Personalized Care
How is privacy protected when treatment uses so much personal information
Privacy depends on process, not slogans. A serious executive program should use strict confidentiality practices, clear consent boundaries, limited information sharing, and disciplined handling of devices, records, and outside communication. High-profile clients often need an additional layer of discretion around family contact, workplace communication, and who is authorized to receive updates.
How does the plan adapt if urgent work demands come up
A good plan expects that issue before admission. Some work contact can be therapeutic if it is structured, time-limited, and supervised within the broader goals of treatment. The mistake is letting work urgency gradually take over the clinical day.
Clients do better when the team helps distinguish between legitimate obligations and reflexive over-engagement. That preserves both treatment integrity and professional credibility.
Why is an integrated team so important in dual diagnosis care
Because co-occurring disorders become messy fast when care is fragmented. A major challenge in personalized planning is coordination across changing risk levels, multiple prescribers, and overlapping mental health and substance use issues. When plans are not managed by an integrated team, they can become clinically incoherent, as discussed in this review of coordination challenges in personalized care.
That matters in real life. If one clinician is treating anxiety, another is addressing substance use, and another is making medication changes without a unified strategy, the client often receives mixed signals. An integrated team keeps one coherent formulation in place and adjusts it as the clinical picture changes.
For families and professionals looking for discreet, high-accountability residential care, Reflections offers a luxury dual-diagnosis setting built around individualized treatment planning, private rooms, appropriate electronics access, and continuing care that respects both recovery and professional life.
Powered by Outrank app









