Some executives reach the end of the day physically exhausted and mentally overclocked. The phone is still active, the inbox is still moving, tomorrow's decisions are already loading, and the body won't follow the schedule the calendar demands. A sleeping pill finds its way into that routine. It starts as a practical fix for travel, a board cycle, a deal sprint, or a period of relentless stress.
Then the pill stops feeling optional.
For high-functioning professionals, that shift is easy to rationalize. The person is still closing transactions, still leading teams, still showing up polished and composed. From the outside, nothing appears to be falling apart. Inside, sleep has become chemically negotiated, evenings revolve around access to medication, and the fear of a pill-free night begins to shape behavior more than is often realized.
That pattern isn't rare. According to 2020 CDC data summarized here, nearly one in five American adults use sleep medication, and stopping can trigger a rebound effect marked by increased wakefulness that keeps people trapped in a cycle of dependence. For a professional whose performance depends on judgment, memory, composure, and timing, that cycle can become costly long before it becomes obvious.
Recovery has to match the life being protected. For executives, founders, attorneys, physicians, investors, and public-facing leaders, treatment isn't about stepping away from responsibility in a reckless way. It's about regaining control with discretion, clinical rigor, and enough structure to protect health, career, and legacy at the same time.
The Executive's Nightly Ritual That Became a Trap
A familiar version of this story begins with competence, not chaos.
A senior leader starts taking a prescribed sleep aid during a period of genuine sleep disruption. It helps after a transcontinental flight. It helps through earnings week. It helps after months of waking at 3 a.m. with a racing mind. The medication appears to solve a narrow problem, so it earns a permanent place on the nightstand.
Weeks later, the relationship changes. Sleep no longer feels available without it.
Why high performers miss the danger
Executives often assess themselves by visible function. If they're still producing, still presenting well, and still making decisions, they assume the system is intact. Sleeping pill addiction doesn't always announce itself with dramatic external collapse. In a high-performance environment, it often hides inside disciplined routines.
Common examples look deceptively polished:
- Travel is arranged around refill timing. The calendar accommodates medication access before it accommodates recovery.
- Evening events become tactical problems. Dinners, flights, and family obligations are evaluated based on whether they interfere with the pill schedule.
- Sleep anxiety increases. The person becomes less confident in the body's ability to sleep naturally.
- Stress gets outsourced to medication. The pill becomes the off-switch for a nervous system that no longer knows how to downshift on its own.
Poor sleep doesn't erase professional capability overnight. It narrows it gradually, then makes the decline feel normal.
That's one reason this form of dependency can persist for a long time in people with significant responsibilities. Their competence masks the cost. They can still perform, but they're performing on a shrinking margin.
The trap isn't weakness
There's no moral failure in wanting sleep. There's no character flaw in using a medication that originally helped. The problem begins when short-term relief becomes a nightly requirement and the original reasons for insomnia remain unaddressed.
In executive life, those reasons are often layered:
| Pressure point | How it shows up at night |
|---|---|
| Constant decision load | The mind stays in analysis mode |
| High visibility | Fear of being off-form the next day |
| Travel and time shifts | Sleep timing becomes unstable |
| Chronic stress | The body remains activated after work |
| Unresolved anxiety or depression | Sleep becomes lighter, later, or fragmented |
A nuanced response recognizes that dependency often grows in people who are used to solving problems efficiently. The pill worked. That's why it was repeated. But an effective intervention has to do more than remove the pill. It has to restore the ability to sleep, regulate stress, and function without chemical reliance.
For high-profile clients, that work also has to preserve privacy, dignity, and continuity of life. Those aren't luxury extras. They're part of whether treatment is viable at all.
How a Sleep Aid Hijacks Your Brain and Performance
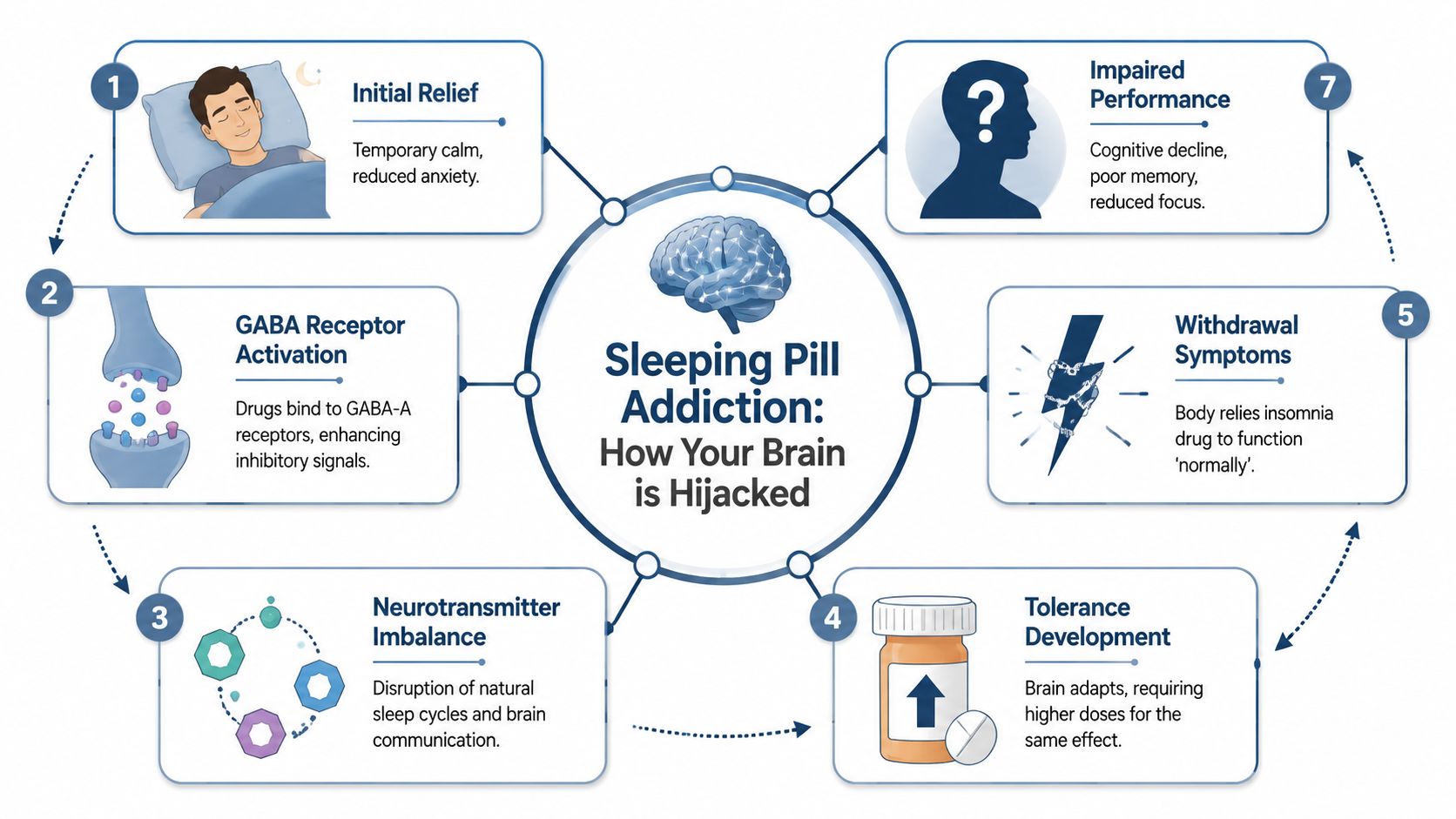
Sleeping pills such as Z-drugs and benzodiazepines create sedation by acting on GABA-A receptors, which inhibit neuronal activity. Physical dependence can develop rapidly, sometimes within just seven days of continuous use, according to this clinical overview. That speed surprises many professionals because the medication still appears to be “working” while dependence is already forming.
What the brain starts doing
The basic mechanism is simple. The medication amplifies the brain's braking system. That produces calm, drowsiness, and a faster transition toward sleep. At first, that can feel like relief. Over time, the brain adjusts to the external signal.
A useful analogy is outsourced leadership. If an outside operator handles a critical function every night, the internal system stops carrying the same load efficiently. With sleeping pill addiction, the brain begins to rely on the drug to initiate sleep instead of maintaining that process naturally.
That shift creates three practical problems:
- Tolerance builds. The original dose may stop producing the same effect.
- Dependence forms. Sleep feels inaccessible without the medication.
- Withdrawal begins when use stops. The brain reacts sharply when the outside sedative signal disappears.
For professionals who've wondered is Ambien a controlled substance?, that question matters because scheduling reflects recognized abuse and dependence risk, not just routine sleep support.
How this shows up at work
Many executives expect sleeping pill addiction to look like obvious intoxication. More often, the damage appears as diminished sharpness. The person isn't necessarily visibly impaired. They're less precise than they used to be.
That can affect performance in ways that matter at the highest levels:
Cognitive drift
A leader who once tracked nuance across a negotiation may start losing detail. Memory becomes less reliable. Important context slips. Follow-through depends more heavily on assistants, notes, or repeated review.
Judgment under pressure
Sedative dependence can blunt the speed and quality of judgment. The person still makes decisions, but the edge is softer. Timing worsens. Complex calls feel heavier. Risk assessment may become either too cautious or oddly inconsistent.
Emotional regulation
Sleep medication dependence doesn't only affect nighttime. It can alter how stress lands the next day. That often means a shorter fuse, flatter affect, more internal agitation, or a growing inability to recover from routine friction.
Practical rule: If a sleep aid is protecting tomorrow's performance in theory but degrading memory, focus, or emotional steadiness in practice, it's no longer functioning as a solution.
The hidden executive cost
High-level work depends on subtle capacities. Pattern recognition. Strategic patience. Controlled communication. Flexible thinking. Those capacities deteriorate before a person becomes visibly unwell.
That's why sleeping pill addiction is so disruptive in professional populations. It doesn't usually take away the ability to work first. It takes away the ability to work at one's natural level. For a founder, partner, surgeon, or C-suite executive, that difference can shape reputation long before anyone uses the word addiction.
Recognizing Addiction in High-Functioning Professionals
A high-functioning professional can meet deadlines, preserve appearance, and still have a serious problem. In this population, sleeping pill addiction often hides behind structure, income, and social credibility. The warning signs tend to be behavioral and psychological long before they become visibly catastrophic.
Clinical estimates suggest about 30% of people who take prescription sleeping pills develop an addiction, marked by behaviors such as tolerance, withdrawal, and spending excessive time seeking or using the drug despite negative consequences, according to this review of sleeping pill addiction.
Red flags that don't match the stereotype
Executives rarely identify with the caricature of addiction. They're more likely to notice smaller shifts and explain them away as stress management. That's what makes honest pattern recognition so important.
A concerning profile may include:
- Dose creep behind the scenes. The medication is used a little earlier, a little more often, or in slightly higher amounts than originally intended.
- Preoccupation with supply. Running low creates outsized anxiety. Travel plans, assistant tasks, or pharmacy logistics start revolving around access.
- Use despite clear downsides. Morning fog, memory issues, irritability, or reduced creativity are noticed but tolerated.
- Private rule-breaking. The person takes “just enough extra” after a difficult night and tells themselves it doesn't count.
- Reliance as a coping strategy. The pill is no longer only for sleep. It's tied to stress, dread, loneliness, post-adrenaline crash, or emotional shutoff.
A more executive-specific self-audit
The most useful question isn't “Has life collapsed?” It's whether freedom has narrowed.
| Subtle sign | What it often means |
|---|---|
| The prescription feels psychologically non-negotiable | Dependence is extending beyond symptom management |
| Strategic thinking feels less fluid | Sedation, poor sleep quality, or withdrawal may be interfering |
| Personal travel requires hidden planning around medication | The substance is shaping life choices |
| There's mounting fear about sleeping unaided | Confidence in natural sleep has been lost |
| Work is still intact, but resilience is worse | Function is being maintained at increasing internal cost |
That pattern often overlaps with anxiety. In some cases, the sleeping pill is part of a larger cycle involving tension, panic, racing thoughts, or benzodiazepine misuse. A clinically useful overview of that overlap appears in this page on benzodiazepine misuse and anxiety treatment.
Many professionals don't ask, “Am I addicted?” They ask, “Why can't I trust myself to sleep anymore?” That's often the more revealing question.
What denial sounds like in this population
Denial in a high-achieving person is usually polished. It sounds reasonable. It may even sound responsible.
Typical internal narratives include these:
- This is temporary, even when use has become routine.
- Work is too demanding to change anything right now.
- It's prescribed, so it can't be a real addiction.
- Nothing is falling apart, so treatment would be excessive.
- Stopping would be worse for performance than continuing.
Those beliefs keep people stuck because they compare the problem only to total breakdown. A stronger comparison is this: current function versus actual baseline capacity. If the medication is now organizing sleep, mood, schedule, and decision quality, the issue deserves clinical attention even if the résumé still looks impressive.
Why Medically Managed Detox Is Non-Negotiable
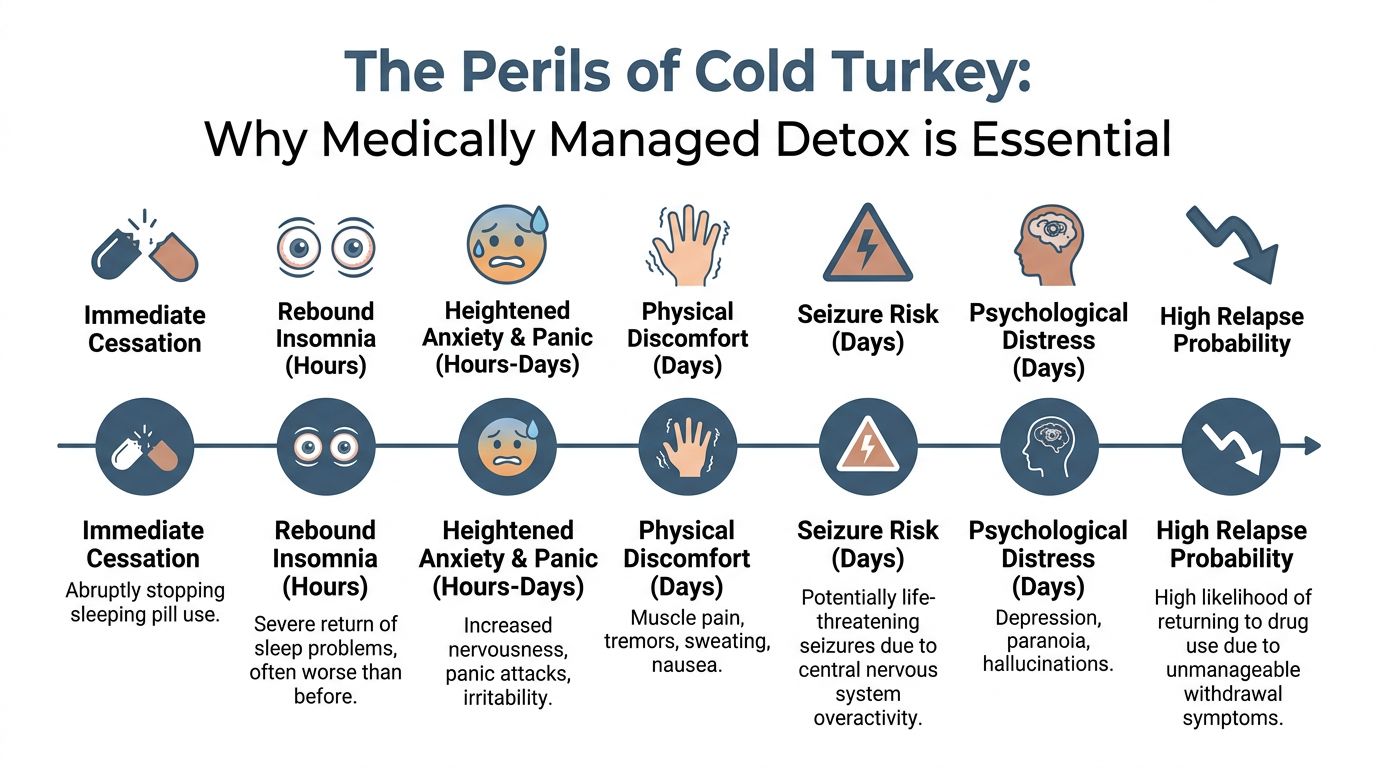
When someone becomes dependent on a sleeping pill, the instinct to stop abruptly is understandable and dangerous. Professionals often try to “white-knuckle” the problem over a long weekend or during a brief gap in travel. That approach fails for two reasons. First, withdrawal can be medically risky. Second, the suffering is often intense enough to drive rapid relapse.
Why stopping alone goes badly
The same medications that force sedation can leave the nervous system overactivated when they're removed too quickly. The result may include severe rebound insomnia, heightened anxiety, agitation, and in some cases seizure risk. That's why detox from sedative-type medications should never be treated like a simple act of will.
For executives, quitting alone creates an additional trap. The person may manage one or two nights with almost no sleep, then face investor calls, patients, clients, court appearances, media obligations, or leadership meetings in a destabilized state. The pressure to regain function quickly pushes them straight back to the pill.
A failed self-detox often deepens the sense of hopelessness. It convinces the person they can't sleep without the medication, when the underlying issue is that the withdrawal process was unmanaged.
What proper detox actually looks like
A clinically managed detox is built to reduce danger and preserve dignity. The process is individualized, gradual, and closely monitored. In a private-pay executive setting, that often means the client doesn't have to choose between medical safety and personal privacy.
A well-run detox generally includes:
- Medical oversight around the clock. Withdrawal symptoms can change quickly, especially with sedative medications.
- A taper rather than abrupt cessation. Gradual reduction is often necessary to lower acute risk and make symptoms more tolerable.
- Private accommodations. A personal room supports sleep stabilization, discretion, and reduced environmental stress.
- Symptom management. The team can address anxiety, insomnia distress, and physical discomfort without improvisation.
- Immediate transition into rehabilitation. Once the body is stabilizing, treatment can begin on the factors that led to dependence.
A concise overview of what withdrawal can involve is available in this internal resource on detox side effects.
The goal of detox isn't to prove toughness. It's to exit dependence safely enough that the person can continue into real treatment.
Why luxury matters here
For high-end clientele, comfort isn't cosmetic. It influences whether a medically necessary process is tolerable. A private room in detox reduces overstimulation and protects confidentiality. A discreet environment lowers the risk of workplace or social exposure. The ability to receive care without being folded into a chaotic setting often makes the difference between entering treatment and postponing it again.
That's especially relevant for executives who can't fully disappear. Some need carefully managed access to phones or laptops. Some need confidential coordination with a spouse, attorney, or physician. Some need a setting where status is irrelevant but privacy is respected.
Detox is the threshold decision. If it's handled poorly, everything after it becomes harder. If it's handled with precision, the client can move from fear and instability into treatment with the nervous system protected instead of shocked.
Beyond the Pill Treatment for the Root Cause
Detox addresses dependence. It doesn't resolve the machinery that made the pill feel necessary. If treatment stops at abstinence, the original drivers of insomnia and overreliance usually remain intact. For professionals, those drivers often include chronic stress activation, anxiety, depression, trauma, grief, burnout, perfectionism, or an inability to disengage from cognitive overwork.
Sleep disruption itself deepens the risk. Research reviewed in this article on sleep and substance use describes sleep disruption as an independent risk factor for substance abuse and relapse, with poor sleep increasing craving and biasing the brain toward drug-seeking as a coping response. That's why effective care has to treat insomnia and substance use together, not as separate issues.
Rebuilding sleep instead of chasing sedation
Many people entering treatment have forgotten what normal sleep pressure feels like. They assume sleep is something that has to be induced. One of the most important interventions is teaching the brain and body how to sleep again without negotiating with a pill bottle.
CBT-I is central to that process. It targets the learned habits and beliefs that keep insomnia in place. That includes fear of sleeplessness, compensatory routines, clock-watching, inconsistent sleep behaviors, and the mental association between bed and struggle.
In practical terms, this means treatment works on:
- evening routines that keep the nervous system activated
- thought patterns that turn one bad night into panic about the next
- conditioned dependence on medication as the only path to rest
- rebuilding confidence that sleep can return naturally over time
Treating the emotional engine underneath
For many executives, sleeping pill addiction isn't only about sleep. It's about state management. The medication may be doing several jobs at once. It may numb the post-performance crash, suppress intrusive thoughts, mute grief, settle panic, or create distance from unresolved trauma.
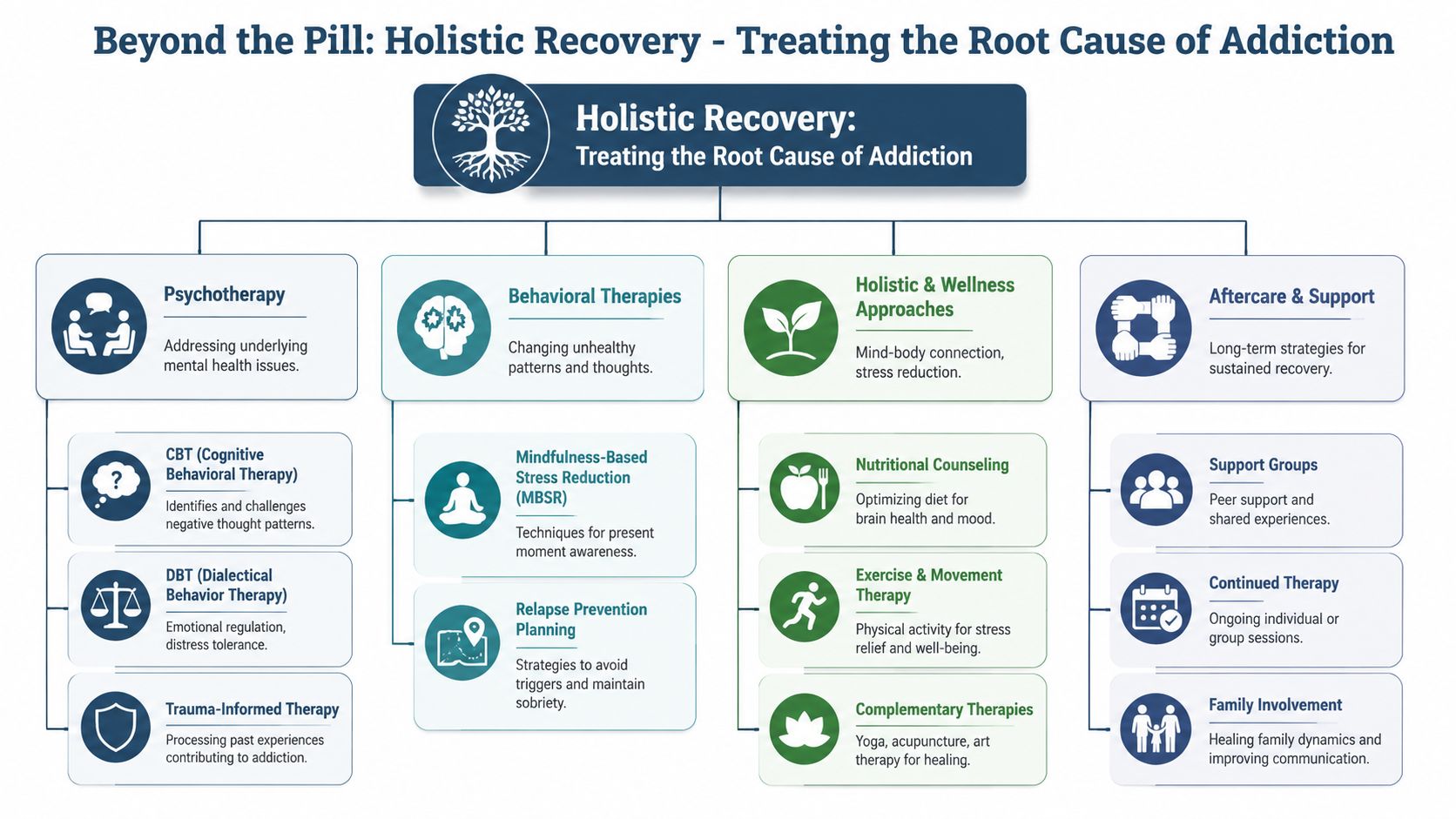
That's why high-quality treatment uses multiple modalities rather than a single counseling model.
Cognitive and behavioral work
Cognitive approaches identify the beliefs that keep both insomnia and substance use alive. Behavioral work interrupts rituals, avoidance patterns, and conditioned cues linked to nighttime medication use.
DBT and stress tolerance
Dialectical Behavior Therapy can be especially useful for professionals who are externally controlled and internally overloaded. It builds distress tolerance, emotional regulation, and skills for managing activation without immediately medicating it away.
Trauma-informed therapy
Some clients can't sustain sleep because the nervous system doesn't experience nighttime as safe. Others carry old trauma into present-day high performance, then use sedatives to shut down what hasn't been processed. In those cases, treatment has to be careful, structured, and trauma-informed rather than merely symptom-focused. This overview of trauma-informed therapy explains why that lens matters in recovery.
A sleeping pill can suppress a symptom. It can't resolve grief, trauma, panic, burnout, or the chronic overactivation that taught the body to fear stillness.
Dual diagnosis is where serious treatment separates itself
Executives with sleeping pill addiction often have a co-occurring mental health condition, even if they've never named it that way. Sometimes it's longstanding anxiety hidden inside achievement. Sometimes it's depression covered by performance. Sometimes it's trauma in highly functional clothing.
A strong dual-diagnosis approach asks better questions:
- What made sleep fragile in the first place?
- What emotional state is the medication managing?
- What happens internally when the client tries to stop?
- Which psychiatric symptoms are primary, and which have been intensified by the medication cycle?
Without that level of assessment, treatment can become too shallow. The person detoxes, returns home, encounters the same mind, the same stress, the same night, and reaches for the same solution.
What tends to work and what usually doesn't
A useful distinction for professionals is this:
| What tends to work | What usually doesn't |
|---|---|
| Gradual tapering with medical support | Abrupt self-discontinuation |
| CBT-I and behavior change around sleep | Hoping abstinence alone restores sleep |
| Dual-diagnosis treatment | Treating insomnia and mental health separately |
| Trauma-informed care when indicated | Forcing insight without stabilization |
| Ongoing relapse prevention | Assuming detox completed the problem |
The core task is restoring internal regulation. When treatment does that well, sleep becomes less of a nightly referendum on control, and recovery stops feeling like deprivation. It starts feeling like regained capacity.
The Modern Executive Rehab Experience
High-performing clients often delay treatment because they picture surrendering control, losing privacy, and disappearing from professional life in a way that creates more damage than the addiction itself. That image is outdated. A well-designed executive program is structured around clinical depth, confidentiality, and continuity.

According to this overview of executive luxury rehab, programs of this kind can cost over $1,000 per day, reflecting personalized clinical teams and continuous access to advanced care rather than décor alone. In the executive tier, the investment is tied to discretion, staffing, and treatment quality.
What clients actually need from the setting
For a senior professional, environment is part of treatment. A chaotic or impersonal setting creates friction at the exact moment stability is needed. A high-end residential model is designed to remove unnecessary noise and support focused work.
That usually includes these practical features:
- Private rooms in detox and residential care. Sleep stabilization, personal privacy, and decompression all improve when the client has a private suite rather than a shared room.
- Small census. Executive programs may keep only eight to twelve clients at a time to strengthen confidentiality and staff access, as described in this executive rehab guide.
- Electronics access. Some professionals can keep cell phones and laptops with appropriate boundaries so they can continue handling critical obligations.
- Highly credentialed teams. Specialized care requires more than generic counseling. It depends on experienced psychiatrists, psychologists, therapists, and addiction specialists working in coordination.
How treatment can coexist with responsibility
The fear many professionals carry is simple. If they leave to get help, everything will unravel. In reality, a structured residential stay often prevents a larger unraveling later.
A typical private residential stay for professionals ranges from 30 to 90 days, with longer care supported when clinically indicated, according to this discussion of private executive rehab. That window is long enough to move beyond physical stabilization and begin real cognitive, behavioral, and psychiatric work.
A strong executive program doesn't encourage nonstop work during treatment. It creates appropriate boundaries. The client may have designated times to manage urgent responsibilities, coordinate with key stakeholders, or remain in limited contact with a company, family office, practice, or legal team. The difference is that work is no longer allowed to swallow the treatment process whole.
In executive treatment, privacy and access aren't indulgences. They're operational requirements that make serious treatment possible for people with real-world obligations.
What a day often feels like
The rhythm of an executive residential program should feel intentional, not institutional. The client wakes in a private room, not a shared unit. Medical and psychiatric needs are addressed in real time. Therapy is individualized. Group work is clinically relevant rather than generic. The environment is calm enough for the nervous system to settle.
A high-end experience also respects status without catering to ego. The point isn't luxury for its own sake. The point is reducing friction so the client can engage fully in treatment while protecting confidentiality and preserving core professional commitments.
That distinction matters. For C-suite leaders and other public-facing professionals, entering rehab can be a strategic act of preservation. It protects cognitive function, physical health, family stability, and long-term reputation better than continuing an addiction that erodes all four.
Integrating Recovery into a High-Performance Life
Leaving residential treatment isn't the finish line. It's the moment recovery has to become livable. For professionals, that means building a post-treatment structure that protects sleep, reduces relapse risk, and fits the demands of a high-performance life without drifting back into the same nightly dependence.
The transition works best when aftercare is specific. “Be careful” isn't a plan. A real plan identifies the pressure points waiting at home and addresses them before they become emergencies. That often includes ongoing individual therapy, psychiatric follow-up when appropriate, sleep-focused behavioral work, relapse prevention planning, and a clear protocol for travel, high-stress periods, and major work events.
The return to work needs design
Professionals do better when re-entry is staged rather than impulsive. That may mean tightening evening commitments, protecting sleep windows, limiting unnecessary travel for a period, and identifying the exact triggers that previously drove medication use. The issue usually isn't ambition itself. It's unstructured overexposure to the same conditions that taught the nervous system to rely on a pill.
Important aftercare anchors often include:
- Continued therapy. The person keeps working on anxiety, trauma, mood, perfectionism, or stress regulation after discharge.
- Sleep protection. Evening routines, schedule boundaries, and CBT-I principles stay active once normal life resumes.
- Support accountability. Regular contact with trusted clinicians, peer support, or alumni programming reduces isolation.
- Family involvement. Loved ones understand the recovery plan and stop reacting only when there's a crisis.
Family and trusted allies matter
High-level professionals often try to contain everything privately, but secrecy is one of addiction's best protections. Family therapy or selected involvement from a spouse or trusted support system can help restore honesty, reduce enabling, and create a home environment that supports recovery instead of passively accommodating the old cycle.
The strongest long-term outcomes usually come from alignment. The client understands the relapse pattern. The treatment team has a continuation plan. Family or trusted allies know what to watch for. Work responsibilities are managed with more discipline, not less.
Recovery doesn't require a smaller life. It requires a more deliberate one. For an executive, that can become an advantage. The same traits that built success, discipline, foresight, and willingness to invest in expert guidance, can also support lasting freedom from sleeping pill addiction when they're directed toward health instead of concealment.
Reflections provides discreet, California-licensed, Joint Commission-accredited luxury treatment for adults dealing with sleeping pill addiction and co-occurring mental health concerns. With private rooms in both detox and residential care, a highly accredited multidisciplinary team, appropriate access to electronics for clients who need to stay engaged with career obligations, and individualized care designed for executives, C-suite leaders, and other high-functioning professionals, the program is built for people who need clinical excellence without sacrificing privacy or continuity. A confidential conversation can help clarify options, timing, and the right level of care. Learn more at Reflections.









