A familiar pattern plays out behind polished calendars and closed office doors. A senior executive keeps performing, keeps showing up, and keeps delivering. Yet sleep is thinner, patience is shorter, concentration is less reliable, and the nightly drink, pill, or other substance stops feeling optional.
From the outside, nothing looks dramatic. From the inside, everything takes more effort.
For high-achieving professionals, depression and substance use rarely look like a public collapse. They look like a slow narrowing of life. Work stays intact just long enough to hide the problem. Reputation delays recognition. Income creates buffers. Intelligence helps with rationalization. By the time family members or colleagues realize something is wrong, the person may already be carrying two intertwined conditions at once.
The Executive Challenge with Depression and Substance Use
A high-functioning professional often doesn't say, “Something is seriously wrong.” The language is usually more controlled than that. It sounds like burnout, irritability, insomnia, loss of edge, or “just needing something to turn the brain off at night.”
That distinction matters. Many executives keep operating while depression and substance use subtly reinforce each other. The person still makes presentations, closes deals, manages teams, and answers messages at midnight. The cost shows up elsewhere. Emotional flatness at home. Rising dependence on alcohol after meetings. Medication misuse to sleep, focus, or calm down. A growing inability to recover between work demands.
This isn't a fringe issue. A national review notes that 33.0% of adults, about 86.6 million people, had either a mental illness or a substance use disorder in the past year in the United States, according to the National Institute on Drug Abuse review summarizing recent national data. In an executive population, the presentation is often more hidden, not less serious.
Why success can delay treatment
Professional achievement creates a dangerous illusion. If someone is still functioning, people assume the problem can't be severe. That assumption fails constantly in dual-diagnosis care.
Executives also face pressures that make disclosure harder:
- Visibility risk means they worry about reputation, licensing, investor confidence, or leadership standing.
- Identity attachment makes rest feel threatening. If performance has defined self-worth for years, stepping back can feel intolerable.
- Access to resources can prolong concealment. Private travel, flexible schedules, and financial means often make it easier to hide worsening patterns.
Clinical reality: Strong performance does not rule out serious illness. It often delays recognition of it.
For professionals in medicine and related fields, burnout can be part of the picture but not the whole picture. This essential guide for medical professionals is useful because it helps separate occupational strain from deeper mental health and substance-related concerns that need direct assessment.
The right response isn't shame. It's strategy. For a high-level professional, seeking confidential dual-diagnosis treatment is often the most responsible decision available. It protects health, judgment, family stability, and the career the person has spent years building.
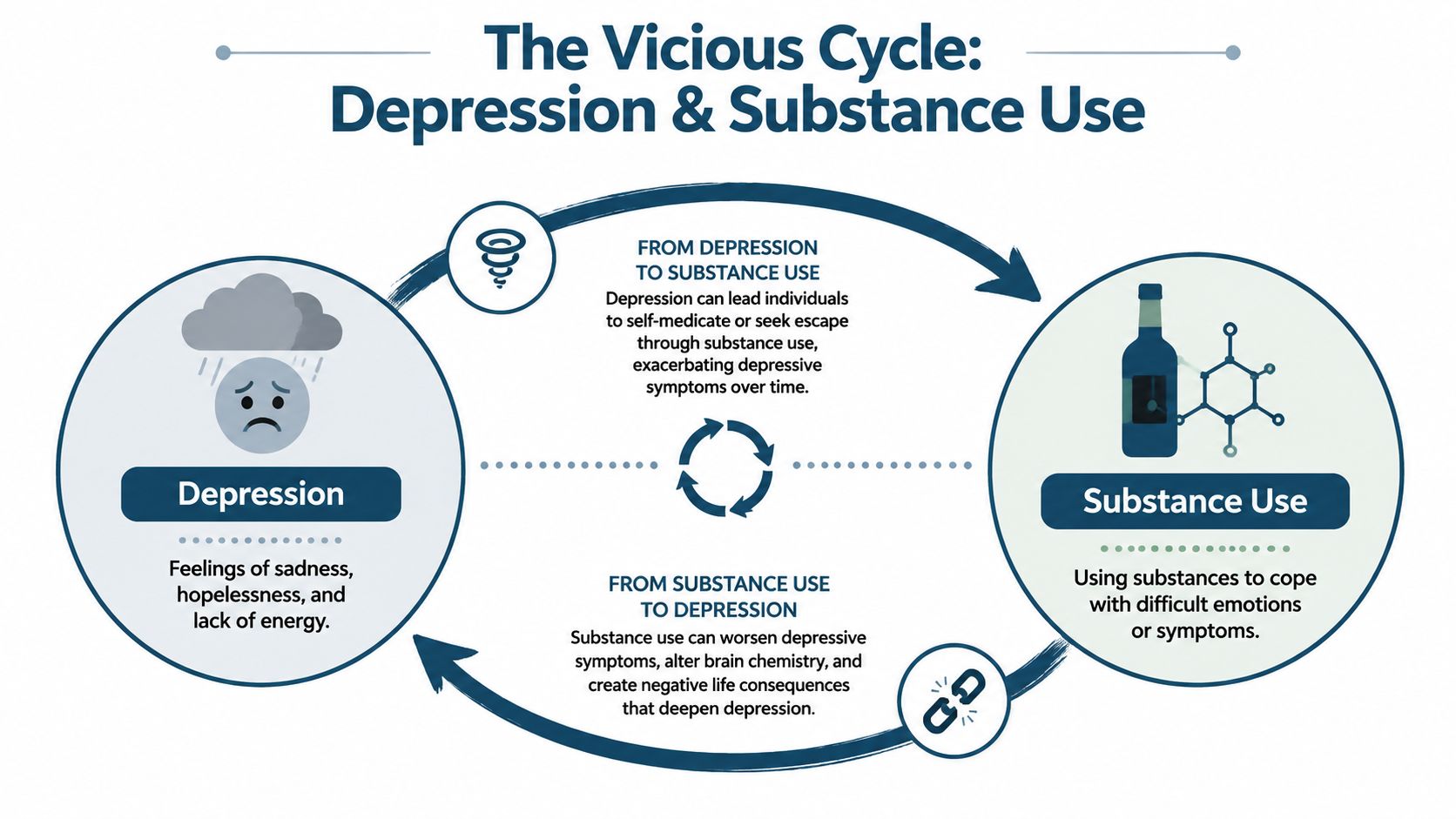
Understanding The Vicious Cycle
A common executive pattern looks like this: alcohol to shut off a racing mind after a late flight, a sedative to force sleep before an early board meeting, a stimulant to stay sharp the next morning, then rising irritability, flat mood, and poorer judgment by the end of the week. The person still performs. The margin for error gets smaller.
Depression and substance use reinforce each other in ways that can be hard to spot from the outside. Low mood, agitation, numbness, hopelessness, and insomnia push a person toward fast relief. Alcohol may quiet intrusive thoughts for a few hours. Sedatives may slow the body down. Stimulants may create a short burst of focus. Cannabis may blunt stress. The relief is real, and short-lived.
Then the cost shows up.
Sleep quality drops. Mood becomes less stable. Anxiety rises. Motivation falls. Shame grows as the person sees the pattern and keeps repeating it anyway. For high-responsibility professionals, that can lead to a private system of chemical compensation: one substance to perform, another to recover, and another to sleep. Over time, the brain and the daily routine start depending on that cycle.
How each side keeps the other active
Depression often drives substance use through a few predictable channels:
- Relief seeking. The goal is often not intoxication. The goal is to feel less awful, less tense, or less emotionally exposed.
- Performance preservation. Professionals may use substances to stay socially polished, sleep on command, reduce panic before presentations, or keep working through exhaustion.
- Avoidance of painful emotion. Grief, fear, loneliness, and self-criticism stay untreated while substances do the regulating.
Substance use then worsens depression in different ways:
- Sleep and brain function change. Even if a substance seems to help at night, rebound insomnia, early waking, and poorer sleep architecture often follow.
- Daily consequences accumulate. Secrecy, irritability, conflict at home, missed details, and inconsistent follow-through feed guilt and hopelessness.
- Confidence erodes. Once a person feels unable to reliably stop, cut back, or function without a chemical assist, depression often deepens.
This overlap is common. The National Institute on Drug Abuse overview of co-occurring conditions notes that about half of people who experience a mental illness during their lives will also experience a substance use disorder, and vice versa.
In practice, trying to treat only the depression or only the substance use usually leaves the cycle intact. That is one reason specialized care for high-functioning professionals with addiction and co-occurring conditions needs to address mood, sleep, stress physiology, work demands, and substance use at the same time.
What usually fails
A narrow plan often breaks down because it misses the trade-offs high performers are already making.
| Approach | Why it falls short |
|---|---|
| Treating depression without a careful substance use assessment | Alcohol, cannabis, stimulants, and sedatives can mimic, worsen, or hide psychiatric symptoms |
| Relying on discipline and willpower | High self-control can delay help, but it does not resolve insomnia, mood instability, or compulsive use |
| Waiting for a visible collapse | Many professionals deteriorate privately while keeping income, title, and outward credibility intact |
| Arguing about which problem came first | Effective treatment can begin before the timeline is fully clear |
The practical question is not which condition deserves more blame. The practical question is what will interrupt both without blowing up a career, a family system, or a professional reputation.
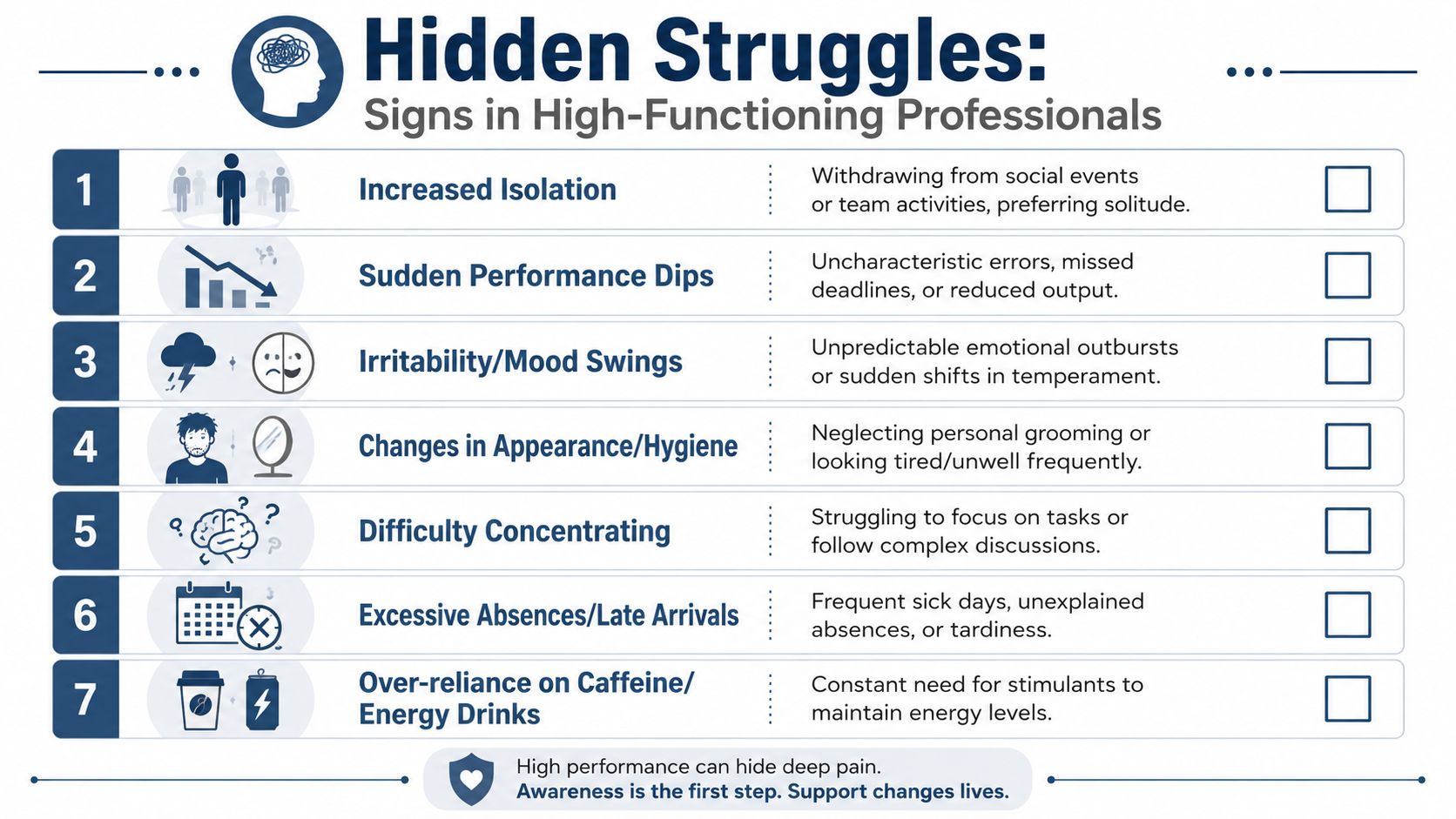
Recognizing The Signs in High-Functioning Professionals
In high performers, the signs are rarely stereotypical. There may be no obvious intoxication, no missed mortgage payment, no dramatic public incident. The person often looks intact because the collapse has been postponed by discipline, status, and routine.
What shows up first is usually a change in pattern. Sharp thinking becomes inconsistent. A once-composed leader becomes unusually reactive. Social confidence turns into withdrawal. The professional still works, but not with the same steadiness, clarity, or range.
What family and colleagues often notice first
The most important clues are behavioral, not dramatic. They include:
- Shorter emotional fuse in meetings, especially under ordinary stress that used to be manageable
- Boom-and-bust productivity where periods of intense output are followed by exhaustion, avoidance, or disappearing
- Reliance on substances to regulate transitions, such as drinking to end the day or using medication to face presentations, travel, or sleep
- Pulling back from relationships while insisting everything is fine
- Loss of pleasure in things that once mattered, including family time, exercise, travel, or professional wins
- Subtle decline in self-care, often masked by expensive routines or polished appearances
- More secrecy around schedule, mood, or consumption
A useful comparison helps here. Stereotypes suggest addiction means visible chaos and depression means obvious sadness. In executives, it often looks more like irritability, detachment, overwork, and private dependence.
Why these patterns can be easy to dismiss
Many professionals explain symptoms in ways that sound reasonable. They blame stress, jet lag, pressure, age, leadership burden, or a difficult quarter. Sometimes those explanations are partly true. They just aren't the whole story.
The risk starts earlier in life than many families realize. Among adolescents with a past-year major depressive episode, 28.4% used illicit drugs, compared with 11.6% of adolescents without a major depressive episode, according to the SAMHSA 2023 NSDUH highlights. Patterns of coping established early can later hide inside successful adult lives.
High functioning doesn't mean healthy functioning. It often means the person has become unusually skilled at operating while unwell.
For readers looking specifically at career-preserving options, this overview of high-functioning professional addiction treatment helps clarify what specialized care can look like when privacy, performance, and continuity all matter.
The Unique Challenges of Diagnosis
A thorough diagnosis isn't as straightforward as many people assume. In executive populations, the clinical picture is often blurred by intelligence, self-discipline, access to private care, and the ability to present well under pressure.
A physician may hear “low energy, poor sleep, no motivation” and think depression. A spouse may see overwork and think burnout. A colleague may notice drinking and assume that's the whole problem. Each interpretation catches one piece and misses the rest.
Why masking leads to incomplete answers
High-achieving adults are often excellent historians of everyone else's needs and poor narrators of their own decline. They minimize loss of control. They present the most acceptable symptoms. They omit the amount used, the frequency of use, or the role substances play in emotional regulation.
That leads to common diagnostic errors:
- Depression gets treated without a meaningful substance use assessment
- Substance use gets addressed as a bad habit rather than a co-occurring disorder
- Exhaustion and cynicism are labeled burnout when the problem is broader
- Anxiety, trauma, grief, or bipolar-spectrum symptoms remain hidden under the more obvious complaint
Why screening has to go both directions
This isn't a minor concern. A pooled analysis found that among patients with major depressive disorder, the prevalence of any substance use disorder was 25.0%, and alcohol use disorder was the most common subtype at 20.8%, based on the pooled prevalence review in the Journal of Affective Disorders.
That finding supports a simple clinical rule. If depression is present, substance use has to be screened carefully. If substance use is present, mood symptoms have to be evaluated just as carefully.
A polished intake interview can be misleading. The right assessment listens for what the patient has normalized, hidden, or explained away.
For professionals, the best evaluations are detailed enough to separate overlapping factors. Is the low mood primary depression, substance-related mood disruption, unresolved trauma, chronic stress, or some combination? Is the drinking recreational, compulsive, withdrawal-avoidant, or performance-managing? Those distinctions shape treatment. Without them, a person can spend months in care that sounds reasonable and still doesn't fit.
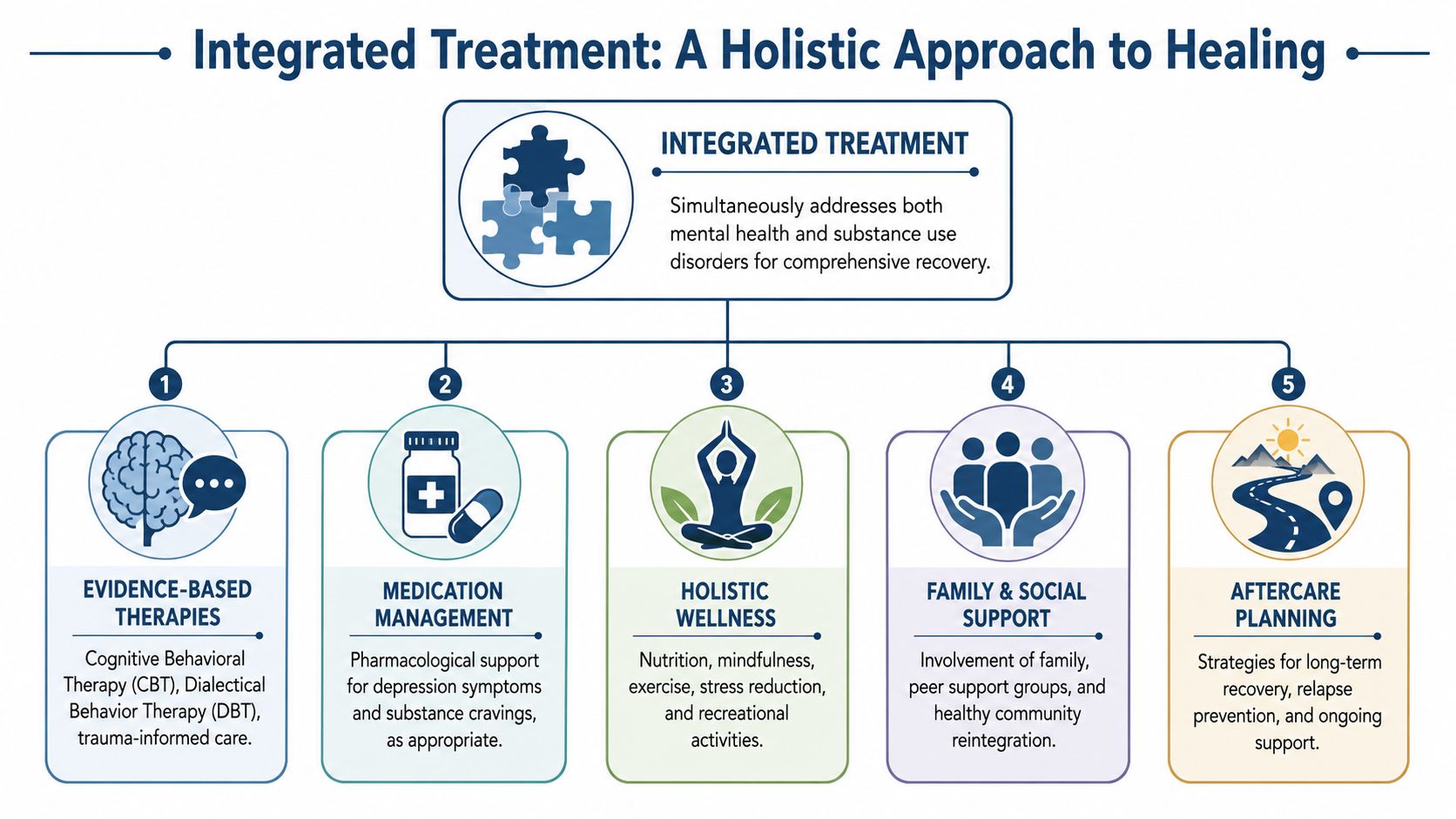
The Power of Integrated Treatment
When depression and substance use are treated separately, the patient often gets trapped in a loop of partial improvement. Mood lifts briefly while use continues. Use drops briefly while depression deepens. The person works hard and still feels stuck.
Integrated care changes the frame. It treats both conditions at the same time, with one coordinated clinical plan.
What integrated treatment includes
Clinical consensus supports this approach. The UNODC notes that comorbid drug use disorders and depression occur at around 50% prevalence in clinical samples, and that treating the disorders together is preferable because sequential treatment is associated with poorer outcomes, as described in the UNODC guidance on comorbidities in drug use disorders.
In practice, integrated treatment usually combines several layers of care:
Psychiatric evaluation and medication review
Medication can be useful, but it has to be precise. Clinicians need to know what substances are involved, what prior medications have helped or failed, and whether a current prescription is helping, sedating, or being misused.Evidence-based psychotherapy
CBT helps identify distorted thinking, relapse patterns, and self-defeating routines. DBT helps with emotional regulation, distress tolerance, and impulsive behavior. Trauma-informed work matters when depression and substance use developed around unresolved pain rather than simple habit.Behavioral restructuring
Executives often need more than insight. They need a new daily architecture for sleep, meetings, nutrition, exercise, communication boundaries, and decompression.Experiential and somatic work
Many high performers live from the neck up. Mindfulness, movement-based work, art therapy, equine work, breathing practices, and guided body awareness can help restore emotional access that has been managed through control and productivity.
What effective care looks like for professionals
A strong program doesn't ask a successful adult to abandon complexity. It addresses it directly.
For example, professionals often need treatment that accounts for ongoing obligations, public visibility, and decision fatigue. That can include coordinated scheduling, private spaces for clinical work, careful medication management, family involvement, and a treatment pace that doesn't confuse intensity with quality. One example is integrated mental health and addiction treatment, which describes a model built around co-occurring care rather than separate tracks.
A practical point often gets overlooked. Recovery routines have to be repeatable in real life. A person who can't sustain basic sleep, exercise, and stress-regulation habits after discharge is more vulnerable when pressure returns. Even a simple outside resource like these practical tips for gym consistency is useful because it reflects a broader truth. Small, repeatable structures beat occasional heroic effort.
Treatment works better when it targets the life the person is actually returning to, not an ideal life with no pressure, no deadlines, and no triggers.
Integrated care also addresses a central question many clients avoid asking directly. If substances have been serving a function, what will replace them? The answer has to be concrete. Better sleep, better emotional regulation, better conflict handling, better boundaries, better treatment of depression. Without those replacements, abstinence becomes deprivation instead of recovery.
What to Expect in Executive Residential Care
For executives and high-profile professionals, the quality of the setting isn't cosmetic. It changes what treatment is possible. A person who won't enter a chaotic environment, share a room, or surrender all professional communication may still accept care if the setting respects privacy, autonomy, and real-world obligations.
That matters because delayed entry is often more dangerous than an imperfect schedule.
The features that actually make a difference
In executive residential care, several elements are especially important:
- Private rooms support rest, confidentiality, and decompression. For clients managing depression, overstimulation and lack of privacy can undermine treatment quickly.
- Discreet clinical operations reduce the fear of exposure. Professionals are more likely to be honest when they trust the environment.
- Electronics access at appropriate times can preserve critical continuity. Some clients need to stay connected to essential work matters, legal communications, or family decisions while still remaining fully engaged in treatment.
- Expert clinical staffing matters because symptom overlap is common. Depression, trauma, anxiety, alcohol misuse, prescription misuse, and executive burnout can look similar on the surface and require very different treatment planning.
- High-quality nutrition, movement, and wellness support help restore the physical systems that mood and substance use have disrupted.
Why luxury matters clinically
A premium setting isn't about indulgence. It's about reducing barriers that keep accomplished people from accepting treatment.
When the environment is calm, private, and professionally run, defenses drop. Patients sleep better. They disclose more. They stay long enough for the work to deepen. Families participate more productively because the process feels organized rather than improvised.
For clients dealing specifically with alcohol use alongside depression, this overview of depression and alcohol addiction treatment shows how a residential track can address both conditions within one coordinated plan.
One further distinction matters for this audience. The goal isn't to help someone disappear from life for a month and then hope they can restart it. The goal is to stabilize health while preserving the parts of life worth returning to. In executive care, career continuity and clinical intensity don't have to be opposing forces when the program is designed correctly.
Your Path Forward to Confidential Care
When a professional or family member suspects co-occurring depression and substance use, the next move should be specific. Waiting for undeniable proof usually means waiting for more damage.
A better starting point is a confidential assessment with a provider that routinely evaluates both mood symptoms and substance use in the same process. The assessment should cover psychiatric history, current use patterns, sleep, medications, trauma exposure, occupational pressure, family concerns, and the practical realities of work obligations. If a center treats only one side of the problem, it may not be the right fit.
How to choose carefully
A few questions help separate serious programs from superficial ones:
- Does the center provide dual-diagnosis assessment from the start?
- Are psychiatrists and licensed therapists directly involved in treatment planning?
- Can the program support discretion, private accommodations, and appropriate communication with work or family?
- Is family work available in a structured, clinically useful way?
- Does the treatment model continue beyond residential care with aftercare planning and ongoing support?
How families can help without making it worse
Families often swing between overprotection and confrontation. Neither works consistently. Productive involvement is calmer and more disciplined.
Families help most when they replace argument with clear observation, boundaries, and a plan for evaluation.
That means describing what they've seen, avoiding amateur diagnosis, and refusing to organize the household around secrecy. It also means choosing a provider capable of handling both the emotional and practical sides of treatment, especially when the patient has a public role, complex responsibilities, or justified concerns about privacy.
The most important decision is often the first honest one. If depression and substance use are both in the room, treatment has to be built for both.
Reflections offers confidential residential dual-diagnosis care for adults dealing with depression and substance use, including executives and working professionals who need private rooms, coordinated psychiatric and therapeutic treatment, family involvement, and appropriate access to electronics during care. Families or prospective clients who need a discreet next step can review options directly through Reflections.









