A high-functioning professional with Borderline Personality Disorder often knows exactly what's at stake before anyone else does. Meetings still need to happen. Teams still expect answers. Family members may see emotional volatility, but colleagues often see output, polish, and control. That split is exhausting.
The wrong treatment model makes that fear worse. Many people delay residential care because they assume it means disappearing from work, surrendering all privacy, and entering a rigid setting that treats a senior executive the same way it treats someone with no outside obligations. That's a mistake. The right BPD residential treatment center for a professional should protect recovery and preserve real-world functioning at the same time.
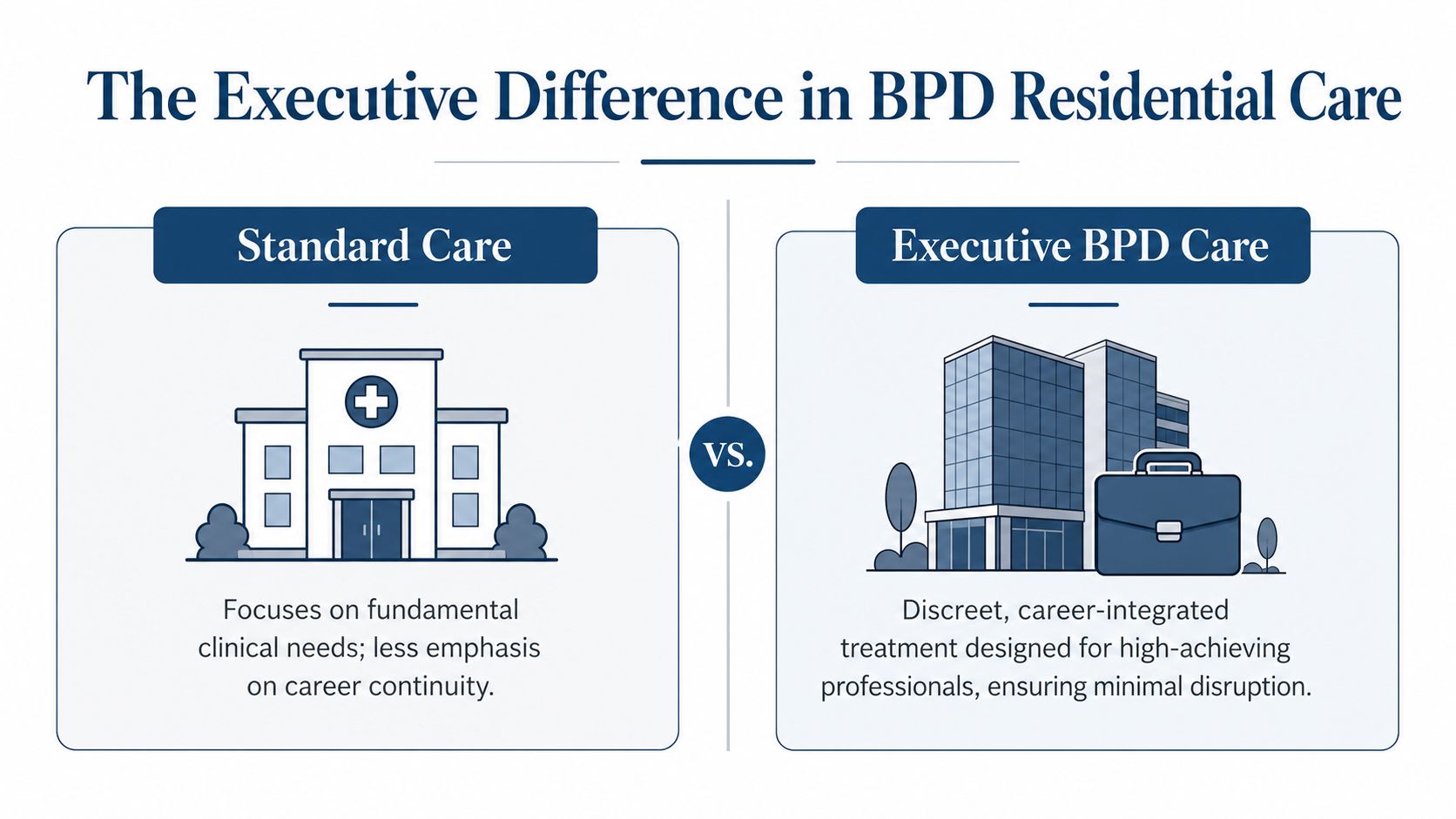
The Executive Difference in BPD Residential Care
A standard residential program may help with stabilization, but it often ignores the practical reality of executive life. A C-suite leader, physician, attorney, founder, or senior operator can't always vanish from every responsibility overnight. Some obligations can be delegated. Some can't.
That's why elite BPD residential treatment centers need an executive model, not a generic one. Privacy matters. Discretion matters. The ability to remain appropriately connected to work matters. Treatment should reduce chaos, not create a second crisis in a person's career.
What executives should expect
Luxury executive rehab facilities differ from standard programs by guaranteeing private rooms for all residents and providing unrestricted cellphone and internet access, which directly supports continuity of work responsibilities for executives and other high-earning professionals, as outlined in this executive rehab overview.
That distinction is not cosmetic. It changes the entire treatment experience.
| Standard clinical model | Executive residential model |
|---|---|
| Shared space and limited privacy | Private room in detox and residential care |
| Restricted communication | Access to cell phones and laptops |
| One-size-fits-all schedules | Structured treatment with room for essential professional obligations |
| Focus on symptom control only | Focus on recovery, discretion, and career continuity |
A high-end program should allow a resident to step out for a confidential call, review a critical document at an appropriate time, or maintain minimal oversight of a company without disrupting therapy. That doesn't mean treatment becomes secondary. It means the program is designed by adults who understand how real leadership roles work.
Why this model works better
Professionals with BPD often arrive burned out from holding too much together for too long. They may have intense emotional swings, unstable relationships, substance use, or a private life that's falling apart while public performance still looks intact. In that situation, shame becomes a major barrier to care.
A serious executive program doesn't punish success. It uses structure, privacy, and clinical precision to help the person behind the title recover.
A premier setting also removes avoidable friction. Private rooms lower interpersonal strain. Electronics access reduces panic about abandoned responsibilities. A calmer physical environment reduces overstimulation. All of that supports treatment engagement.
For readers evaluating options, this is the benchmark for luxury rehab for executives. If a center markets itself to professionals but forces unnecessary disconnection, shared housing, or blanket restrictions that ignore actual responsibilities, it isn't built for executive care. It's built for convenience on the provider side.
Core Evidence-Based Treatments in a Premier Setting
Amenities don't treat BPD. Clinical depth does. A private room and laptop access only matter if the therapeutic work is advanced, intensive, and individualized.
The foundation should be Dialectical Behavior Therapy, paired with other evidence-based modalities that address trauma, distorted beliefs, attachment injuries, and entrenched behavioral patterns. In a premier setting, those treatments aren't delivered as a generic curriculum. They're adapted to the person's presentation, history, and level of functioning.
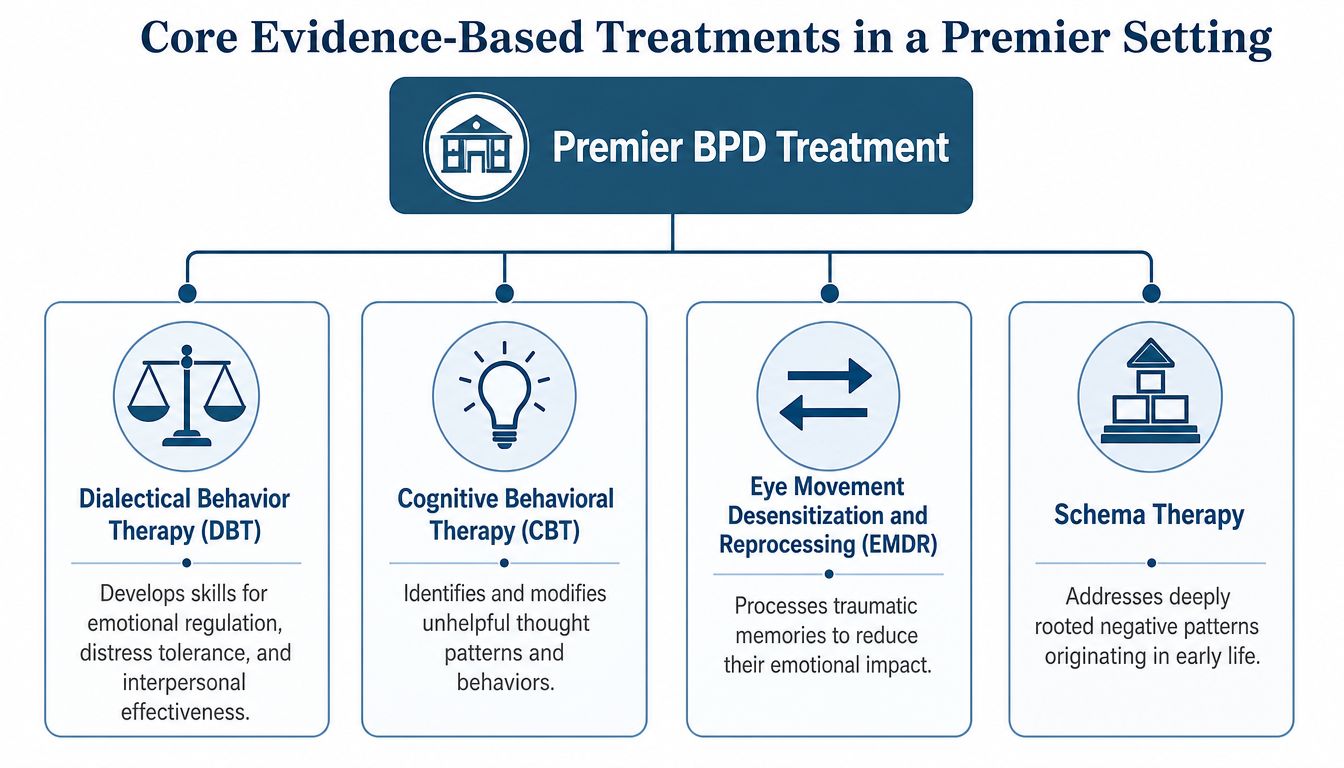
DBT is non-negotiable
Residential treatment that adheres to DBT shows large-effect-size reductions in BPD symptom severity, with Cohen's d ≥ 1.0 for depression and functional disability improvements after just one month of intensive intervention, according to this DBT residential treatment study.
That matters because BPD is not a motivation problem. It's a regulation problem. DBT directly targets the areas that keep professionals trapped in repeated crises:
- Emotion regulation helps reduce abrupt escalation that damages decision-making and relationships.
- Distress tolerance helps the person get through conflict, shame, panic, or urges without impulsive action.
- Interpersonal effectiveness addresses the exact patterns that often sabotage partnerships, leadership dynamics, and family life.
- Mindfulness improves pause, awareness, and behavioral choice under pressure.
A strong residential program should also provide individualized DBT delivery, not just skills groups. That includes one-to-one therapy, real-time coaching, and treatment planning that reflects the patient's actual triggers. A program such as DBT at Reflections is one example of a residential setting that incorporates this modality within a broader dual-diagnosis framework.
Other therapies that should be present
DBT is the anchor, but it shouldn't be the whole building. High-caliber executive treatment often combines several approaches.
- Mentalization-based work helps patients understand their own internal states and interpret other people more accurately. That's essential when a leader swings from overconfidence to paranoia, idealization to rage, or closeness to withdrawal.
- Trauma-informed therapy addresses the developmental and relational injuries that often sit underneath BPD symptoms.
- CBT and schema-focused work help identify automatic beliefs such as “I'll be abandoned,” “I'm defective,” or “I have to control everything.”
- Medication management should be careful and conservative. The goal is stabilization and clarity, not sedation.
Clinical test: If a center talks more about amenities than about how its clinicians apply DBT, trauma treatment, and individualized psychotherapy, it's selling comfort, not treatment.
The best luxury programs understand that “high-functioning” doesn't mean less severe. It often means the symptoms have been organized around achievement, status, and overperformance. That requires a very skilled clinical team.
Navigating Levels of Care for BPD Treatment
Many professionals try to negotiate with severity. They want the least disruptive option, not the right one. That's understandable, but it often prolongs the problem.
BPD care usually falls into three broad levels. They are not interchangeable.
Residential versus PHP versus IOP
| Level of care | What it offers | Best fit |
|---|---|---|
| Residential treatment | Live-in support, daily therapy, immersive structure, constant clinical containment | BPD symptoms are destabilizing work, relationships, safety, or substance use |
| Partial Hospitalization Program | Full clinical days with return home at night | The person needs significant treatment but can remain stable outside the program |
| Intensive Outpatient Program | Several therapy sessions each week while living at home and maintaining more routine | Symptoms are present but manageable without round-the-clock support |
Residential care is the strongest option when daily life has become part of the illness cycle. Home conflict, professional pressure, access to substances, romantic instability, isolation, and secrecy can all keep BPD symptoms active. Removing a person from that loop gives treatment a real chance to work.
Why executives often underestimate their need
A senior professional may still be showing up to meetings, generating revenue, or managing a team. That can create the illusion that outpatient treatment should be enough. It often isn't.
If a person is white-knuckling through the day, unraveling at night, using substances to regulate emotion, cycling through relationship blowups, or constantly threatening to quit, disappear, or explode, outpatient care may be too thin. A weekly appointment can't compete with a relentless environment.
Choosing residential care early is often the fastest route back to stable functioning. Delaying it usually costs more time, more damage, and more disruption.
For executives, the right residential setting doesn't erase work identity. It puts that identity in the proper place. Recovery becomes the primary assignment, while essential career obligations are managed with boundaries instead of panic.
The Critical Role of Integrated Dual-Diagnosis Care
Treating BPD without addressing co-occurring conditions is poor clinical practice. It leaves the most destabilizing drivers untouched.
That's especially true for high-functioning professionals, who often use work performance to mask a deeper pattern of substance use, trauma, anxiety, depression, or all of the above. A center that treats BPD as a stand-alone issue will miss the actual architecture of the problem.

Why dual diagnosis has to be integrated
Public information on BPD residential care often skips the needs of high-functioning professionals, even though over 65% of adults with BPD also have a substance use disorder, as noted in this overview of BPD treatment and co-occurring addiction.
That single fact changes the admissions conversation. If substance use is present, it cannot be handled as a side issue. It shapes mood instability, impulsivity, self-harm risk, sleep, judgment, treatment participation, and relapse vulnerability.
A true dual-diagnosis program should include:
- One unified treatment plan that addresses BPD, addiction, and other psychiatric issues together
- Coordinated psychiatry and psychotherapy, rather than disconnected providers making separate decisions
- Detox capability or clinical withdrawal management when needed
- Therapists who understand both personality dynamics and addiction patterns
- Aftercare planning that continues both mental health and recovery work after discharge
Why professionals need a specialized version
Executives often minimize substance use because they're still functioning publicly. They may frame alcohol, stimulants, sedatives, or other substances as tools for performance, sleep, or emotional shutdown. That framing is common. It's also dangerous.
An executive-focused program has to recognize the role of identity here. The person is often trying to preserve competence, authority, and image while privately losing control. A generic addiction track may miss the shame, secrecy, and performance pressure driving the cycle.
A program with integrated dual-diagnosis treatment is better positioned to treat the full pattern. That includes the emotional volatility of BPD, the reinforcement loop of substance use, and the professional pressures that keep both conditions hidden.
Hallmarks of an Accredited High-Caliber Program
Choosing among BPD residential treatment centers shouldn't come down to marketing language. It should come down to standards. A serious program can explain how it protects safety, reduces dropout, staffs care, involves families, and manages the practical side of treatment.
One warning sign deserves attention. Patients with BPD have center-initiated dropout rates of 26.5% compared with 6.4% for patients without BPD, according to this study on residential treatment dropout. That gap tells a simple story. Generic residential systems often aren't built well enough for this population.
What the gold standard looks like
A high-caliber center should show strength in several areas at once.
Accreditation and licensing
Accreditation matters because it gives families and referring professionals an objective baseline for safety and quality. A licensed residential center with strong accreditation has been evaluated against external standards, not just its own promises.
Senior clinical staffing
BPD is complex. Executive patients are often more complex. They may present with polished communication, legal exposure, substance use, trauma, family strain, and a strong ability to intellectualize distress. That's why staffing should include experienced psychologists, psychiatrists, licensed therapists, and addiction specialists who can work as one team.
Family involvement
The family system often needs treatment too. Not because relatives caused BPD, but because the disorder affects communication, trust, boundaries, enabling, and conflict across the whole household. Good programs use family sessions and educational work to change the environment the patient returns to.
The right question isn't “Is this place comfortable?” It's “Can this team keep a complex patient engaged long enough to do meaningful work?”
Questions that separate serious programs from polished ones
- How does the program reduce premature discharge for BPD patients? Ask for actual protocols, not vague reassurance.
- Who directs treatment? Titles matter less than credentials, experience, and team integration.
- How are work obligations managed without undermining treatment? Executive access should be structured, not chaotic.
- Are private rooms standard in both detox and residential care? For high-profile clients, this matters.
- How are family sessions handled? The answer should be specific.
- What happens after discharge? Strong residential care includes continuing care planning, not just discharge paperwork.
Financial operations also matter more than many families realize. Admissions, verification, billing clarity, and private-pay communication all affect trust and decision-making. For readers trying to understand the administrative side of behavioral healthcare, this guide to RCM best practices is useful context for how competent organizations handle revenue cycle processes transparently.
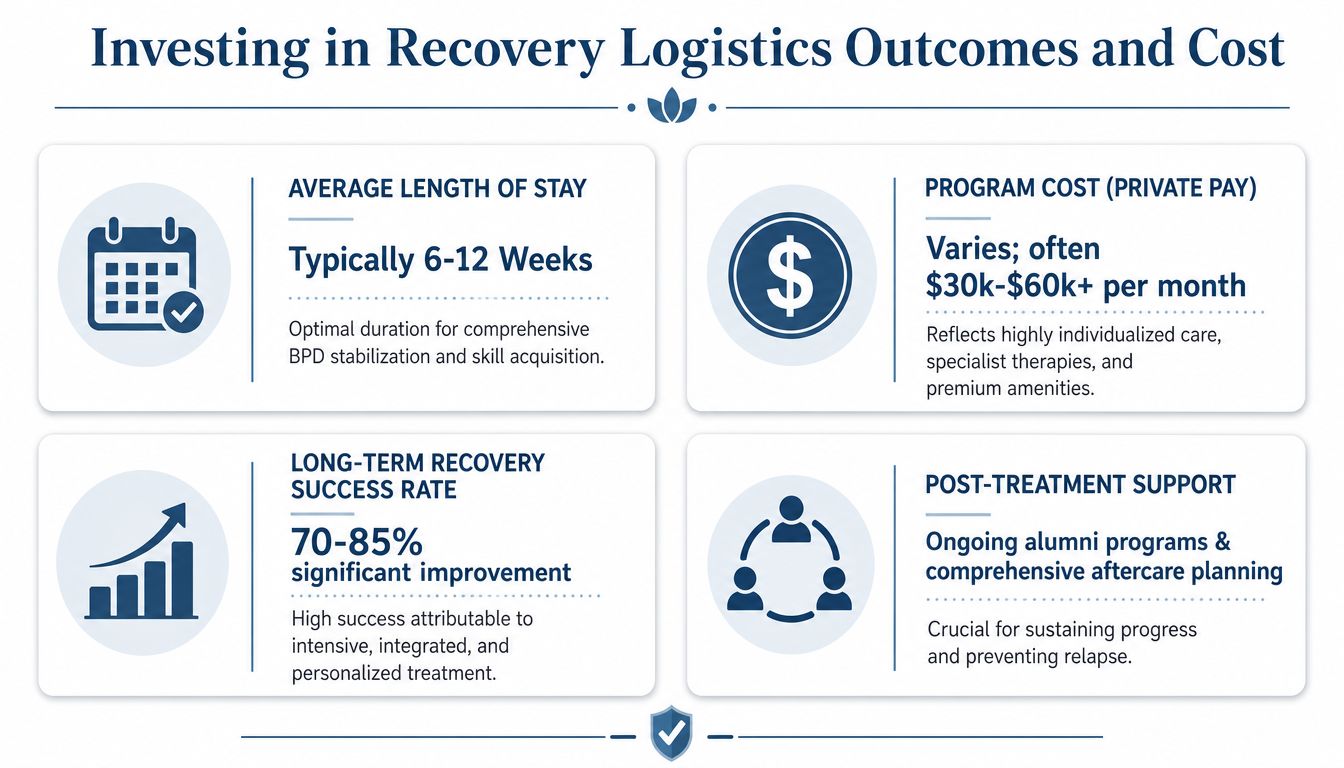
Investing in Recovery Logistics Outcomes and Cost
Elite BPD residential treatment is expensive. That should be stated plainly, not hidden behind vague admissions language. Executive luxury rehab programs typically cost between $80,000 and $150,000 for a standard 30-day residential stay, based on this executive rehab cost overview.
For the right patient, that cost is not irrational. It's often a strategic correction. Untreated BPD can destroy relationships, destabilize companies, trigger legal and financial fallout, fuel addiction, and erode a career that took decades to build.
The return isn't just symptom relief
The central argument for premier residential treatment is simple. It offers a higher level of containment, privacy, and clinical precision during a period when the patient's usual coping system is no longer working.
For executives, the benefits are practical:
- Career protection: A structured pause is often less damaging than an uncontrolled collapse.
- Relationship repair: Intensive treatment can interrupt the repeated patterns that drive separation, distrust, and volatility.
- Substance stabilization: If addiction is in the picture, integrated care addresses it before it deepens.
- Decision-making recovery: Better regulation improves judgment, communication, and consistency.
People often focus on the price tag because it's visible. The hidden costs of not getting effective treatment are usually much larger.
Outcome data matters
The strongest argument for intensive care is that meaningful recovery is possible. Research indicates that 93% of patients with BPD admitted to inpatient or residential treatment settings achieve symptom remission lasting at least two years, according to this report on inpatient and residential BPD outcomes.
That figure should change how families think about residential care. The old idea that BPD is untreatable is outdated. The disorder is difficult, but it responds to serious treatment when the program is structured well and the patient stays engaged.
Residential treatment shouldn't be framed as retreat. For many professionals, it's the most disciplined move available.
Handling the logistics without creating more chaos
The admissions process needs to be managed like any other high-stakes transition. Calmly. Quickly. With confidentiality.
A practical sequence usually looks like this:
- Clinical assessment first. Confirm whether residential care is the right level.
- Work triage next. Identify what must be delegated, what can be paused, and what requires limited direct involvement.
- Family alignment. Spouses, partners, or close relatives need a clear message about the plan and the expected boundaries.
- Financial review. Private-pay treatment requires direct clarity on fees, length of stay, and what's included.
- Aftercare planning from the start. Discharge should not be an afterthought.
For professionals, one of the biggest mistakes is trying to preserve every work function during treatment. That defeats the purpose. Executive-focused residential care should support essential continuity, not ongoing overwork. Cell phone and laptop access are tools, not invitations to stay emotionally unavailable.
What to tell family and colleagues
A concise explanation usually works best. A patient doesn't need to disclose a full diagnosis to every colleague. Many professionals communicate that they're entering a confidential health program and that responsibilities have been delegated for a defined period.
Family members need a different conversation. They need honesty about severity, expectations around communication, and a realistic understanding that recovery requires structure. Not constant reassurance. Not negotiation. Not rescue.
The right center helps organize all of this. It doesn't just admit the patient. It helps contain the disruption around the patient so treatment can begin under stable conditions.
Reflections provides California-licensed, Joint Commission-accredited residential dual-diagnosis treatment for adults who need intensive care in a private setting, including professionals who require private rooms, appropriate electronics access, and coordinated treatment for BPD, substance use, trauma, anxiety, depression, and related conditions. Readers evaluating executive-focused options can review the program directly at Reflections.









